izusek/Getty Images
Amid the debate over reopening schools without draconian restrictions, some of the best case studies from which to draw conclusions are child-care settings that have already been open during the pandemic. A number of child-care facilities for young children never shut down, and a goodly number of camps wound up opening later in the summer for children of all ages. New data show remarkably few cases and no reported clinical problems from those cases.
Emily Oster, an economics professor at Brown University, and Galit Alter, a professor of medicine at Harvard Medical School, created a database of COVID-19 cases from selectively reporting child-care facilities and summer camps at their website, Covid Explained. As you can see from the data of camps, schools, and child-care facilities that are open, the cases are remarkably low:
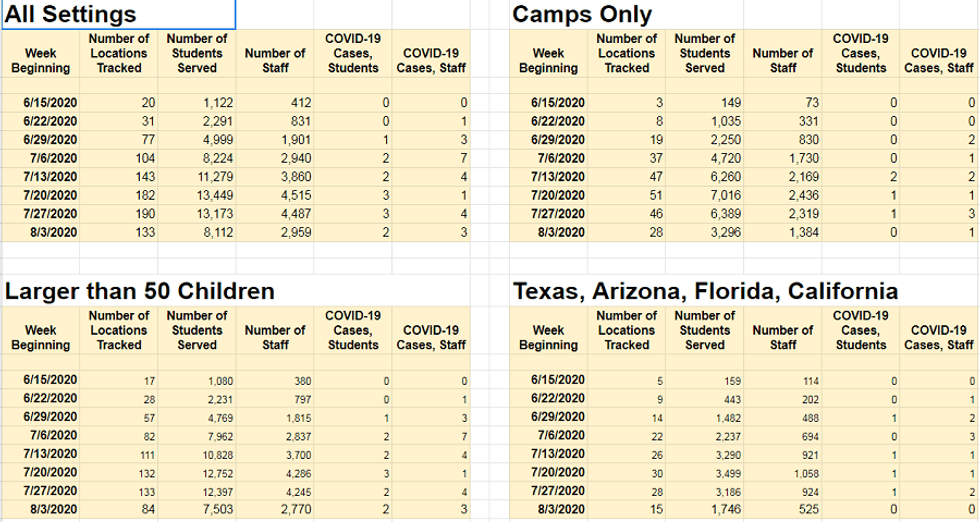
Obviously, this is not a scientific study because the facilities voluntarily participated in this tracking program and they are not randomly sampled. But the size is large enough to get a sense that there really is not a lot of disruption going on, and if not for the panic and mass testing, they probably would never even have known about these few cases. In terms of passing around bugs, this is nothing more or less than we typically see from children's institutions.
My child came back from a backyard camp with a 10-day cold, and my wife and I, as well as many other parents, got that cold. None of us had typical COVID-19 symptoms. One parent decided to get tested, and of course the result was negative. Children pass around colds and flus all the time, and the symptoms are actually more severe than COVID-19 symptoms for almost all children. I could barely get out of bed for two days over the weekend.
We can't allow the discovery of a handful of asymptomatic or mildly symptomatic cases that are far from ever being clinical to shut down a generation of children's education and activities.
On any given day or week, there are a number of kids with colds or even fevers. For the most part, that is actually a good thing and is partially responsible for building up their innate immune systems against more serious threats, such as an acute case of COVID-19. If we created a testing system and ascribed a scientifically scary-sounding name to each ailment, we'd live in a state of paralysis every year.
But this is what we will face in the coming year with mass testing, mass hysteria, and the treatment of every subclinical COVID case as if it's stage 4 cancer. The University of Kentucky has already tested well over 7,000 students, and 0.6% of them (41 students) tested positive. Absent any testing, we probably would not know about a single case, because none of them rose to the level of anything more acute than typical bugs that are passed around.
Last week, one media outlet in New Hampshire published an entire article about a staff member or student of a preschool who tested negative! The Keene, New Hampshire, school closed after two members of the community believed they had exhibited some symptoms of COVID-19. It turns out one of them had strep throat, and the other tested negative for COVID but is still waiting for a second negative test. So now just the onset of a cold that might prompt someone to test is newsworthy and will sow panic as if there is the spread of Ebola in a school. Strep throat is as common as spitballs in school settings and can actually cause serious side effects, but it's something we've always lived with. Why should coronavirus be any different?
What are we going to do with the flu season when even a cough or a sneeze is now a pretext for panic? What's next? A count of papercuts and playground bruises?
Inevitably, the media always focuses on the one exception to the rule, which, when studied properly, is not much of an exception. As the data from Professor Oster shows, even during peak transmission in hot spots, the reporting camp and day care facilities had low numbers of cases. The exception is one camp in north Georgia that the CDC reported on in a published paper, which was frantically touted by the media as a harbinger of doom for school reopening. They found that hundreds of kids and counselors tested positive, which resulted in the closure of the camp a few days after it opened.
But have you read anything in the media about a single one being hospitalized or this outbreak setting off another cluster elsewhere? The Atlanta Journal-Constitution, which later identified the camp as "Camp High Harbor" in Rabun County, reported that "state health officials said they were not aware of any hospitalizations or fatalities stemming from the outbreak." All you will read about are asymptomatic cases, sore throats, and mild fevers. These happen in schools across the country all the time, especially in flu season. But in a country of 330 million, you will find cases like this even in the summer.
Also, based on the information provided in the CDC paper, it's impossible to know who passed COVID to whom. Thus, without evidence to the contrary, we would have to assume that this follows the pattern of every other study indicating children get the virus from adults. We therefore must presume that the counselors passed COVID to the kids and not the other way around or that outbreak this originated from outside the camp.
The counselors were at the facility for four days of training beginning on June 17 before the campers arrived and likely spread it before the campers came, because the camp was shut down shortly afterwards. Campers didn't arrive until June 21, the first symptoms were recognized on June 23, and the camp started closing the very next day through June 27. It's hard to see how the spread occurred among the younger kids and not the older staff.
It's not as if we found any camp in the country that was opened throughout the past six weeks where there was a sudden outbreak that could be traced from child to child. In fact, because we have not found such a case well into August, it's quite clear this outbreak of a camp that was opened for just two days in June was baked into the cake before the kids arrived.
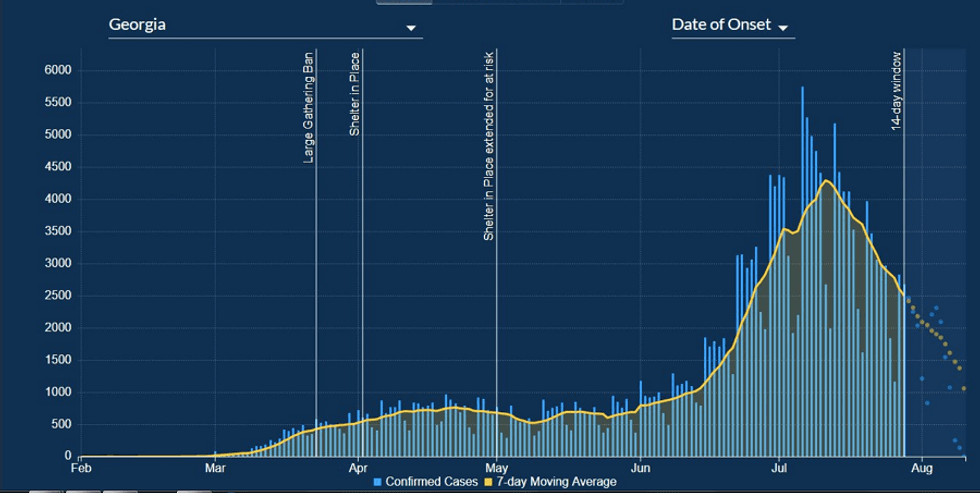
Also, they counted anyone who tested positive 14 days after the closures of the camp. That is from June 27 through July 10. That was during the peak transmission in Georgia, as its daily case count reached its highest levels on July 6. How many of them got it after the camp was already closed – from their parents at home?
As the CDC concedes, "Given the increasing incidence of COVID-19 in Georgia in June and July, some cases might have resulted from transmission occurring before or after camp attendance."
It's truly shocking how the CDC failed to investigate the ages of those first caught with symptoms, which would likely explain why the youngest cohort of campers had the highest attack rate, which as they noted, was quite surprising. It's likely that the counselor that first spread it was the one in charge of the children 6-10.
As for the symptoms, aside from the asymptomatic, a big portion of the other kids had suggestive symptoms. Anyone who has questioned their kids about wellness knows they are extremely suggestive to disease.
"How do you feel, Johnny?"
"I feel good."
"So, no headache or sore throat?"
"Oh, actually yes my head hurts a little."
According to the CDC, out of the 260 who tested positive, 136 cases had available documented symptom data. Among them 26% reported no symptoms, while 74% did report symptoms but "those most commonly reported were subjective or documented fever (65%), headache (61%), and sore throat (46%)."
Since this case was an anomaly, without other available information, one has to question whether there were other anomalous circumstances. We know kids often get other viruses, plus many of the tests produce false positives. In this case, it doesn't appear that other viruses were tested for. For example, it's currently enterovirus season, which affects millions of kids with cold or mild flu-like symptoms every year. How many kids were really asymptomatic, but were co-infected with other mildly symptomatic respiratory viruses that are also contagious and more transmissible from child to child than COVID-19?
This is not a far-fetched assumption. Keep in mind that kids have had their immune systems shielded for several months due to isolation, as I experienced with my children's summer camp and the spread of this wicked cold to my household (as my podcast listeners can attest, with my gutted radio voice). Perhaps those with measurable symptoms of fever (assuming it was measured accurately) were co-infected with the spread of other respiratory viruses that overlapped with COVID-19?
Either way, we live in an era of panic first, ask questions never.