© 2024 Blaze Media LLC. All rights reserved.
We no longer need to rely on unicorn simulation models to predict the threat level of COVID-19. After millions of global cases, we now have reams of hard data. In recent days, two things have become clear: 1) The overall death rate is dramatically inflated with people who died only with COVID-19 – not because of it – especially in nursing homes; 2) Outside nursing homes, the fatality rate is low even for most seniors and shockingly low for younger and healthier people. This destroys politicians’ reasons for pushing the irrevocably harmful actions taken by our government rather than a more strategic and targeted approach.
To begin with, the media and politicians are still promoting high overall infection fatality rates (IFR), such as the World Health Organization’s estimate of 3.4%. But we’ve seen enough random sampling from serological antibody tests, corroborated by hard data from prisons and navy ships, to demonstrate that the virus spread earlier, wider, and more asymptomatically than previously thought, thereby driving the fatality rate much lower. A new analysis averaging all the major antibody tests indicates that the average overall fatality rate (including nursing home deaths) is 0.2%. Why have our policies not been updated to reflect that reality?
This week, Dr. John P.A. Ioannidis published a preprint (before peer review) analysis averaging the fatality rates reflected in the extrapolation of all the serology tests with a sample size larger than 500 and that were randomly sampled (as opposed to health care workers). These tests measure the seroprevalence – the prevalence of antibodies for the virus in a given population – through some degree of random sampling.
Based on these random samples, the Stanford professor of medicine, epidemiology, biomedical data science, and statistics concluded that the fatality rate ranges from 0.02% to 0.40%. That is a range of seven times less deadly or 2.8 times more deadly than seasonal influenza.
The mean IFR is 0.2%, right around the result we saw from the first U.S. serology studies in Santa Clara, Los Angeles, and Miami Dade Counties. That is 17 times less deadly than what the World Health Organization originally predicted and 4.5 times less deadly than the Imperial College study assumed!
The study included data from 12 antibody tests conducted in different countries, from the U.S. and Brazil to China, Japan, Iran, and several European countries. They collectively show that the virus is exponentially more prevalent, often presenting asymptomatically, than the confirmed case tally indicates. Ioannidis further notes that most of these surveys likely understate the number of infections (and therefore overstate the fatality rate) because several of them were of blood plasma donors, who tend to be healthier people.
Also, the virus seems to be particularly widespread in nursing homes, in prisons, and among disadvantaged minorities, which Ioannidis believes were underrepresented in these samples. He noted that this was especially true in the Santa Clara study conducted by his Stanford colleagues, which seemed to disproportionately attract wealthy volunteers.
Nonetheless, he concludes:
Interestingly, despite their differences in design, execution, and analysis, most studies provide IFR point estimates that are within a relatively narrow range. Seven of the 12 inferred IFRs are in the range 0.07 to 0.20 (corrected IFR of 0.06 to 0.16) which are similar to IFR values of seasonal influenza. Three values are modestly higher (corrected IFR of 0.25-0.40 in Gangelt, Geneva, and Wuhan) and two are modestly lower than this range (corrected IFR of 0.02-0.03 in Kobe and Oise).
Ioannides observes that two of the three antibody studies with the higher range were in cities with super-spreading events in the lead-up to the infection peak, and Wuhan had a situation where hospitals were overrun.
Obviously, New York’s experience was an outlier, so the antibody test conducted by the state (which indicates an IFR of at least 0.6% for New York City) was not included in his analysis. He chalks up the more severe outcome in places like New York City and northern Italy to an amalgamation of factors that fed on each other, including: hospitals reaching capacity, large numbers of medical providers becoming infected and spreading it in the hospitals,
use of unnecessarily aggressive ventilation treatment, and in the case of NYC, in particular,
“an extremely busy, congested public transport system that may have exposed large
segments of the population to high infectious load in close contact transmission and, thus, perhaps more severe disease.”
Of course, public transportation was the one thing that was not shut down, even as officials closed outdoor parks and beaches, where every single published study as shown nearly zero transmission.
However, whether we go with a top-line IFR of 0.2%, 0.6%, or even the 0.9% of the Imperial College projection, it fails to account for the most salient characteristic of this virus – that its threat is extremely lopsided. In most countries and states, more than half of all deaths are in nursing homes, and in some states, upwards of 70 percent are – with many of the decedents having already been placed in hospice or end-of-life care. Most of the deaths are tragically within a tiny cohort of the population with a 5%-10% IFR, which is 25-50 times higher than the median.
Take Pennsylvania, for example. Roughly 68 percent of all deaths statewide occurred in nursing homes. At the same time, 58 percent of all deaths were among those over 80 and 70 percent were over 75. In fact, there were more deaths over age 95 (a rare slice of the population) than those under age 60. So how many of those over 75 or 80 who died were outside nursing homes? No state has published such data, but if you do the math and assume that most of the nursing homes deaths were among seniors (a pretty solid assumption), it means that more than 90% of senior deaths were in nursing homes. Thus, the fatality rate even for seniors outside nursing homes is dramatically lower than the top-line numbers suggest.
As I’ve noted before, the nursing homes have appallingly high numbers because of several factors, including a likely overcount of the numbers, the disastrous decision to send positive patients back into the senior homes, and the fact that the median stay of anyone who dies in any nursing homes is just five months. Most seniors outside these homes, while facing an elevated risk over younger people, are much better off than those in these facilities.
What about those younger than 60 or 65? Their death rate is so remarkably low that the risk does not rise above the level of any normal daily activity. In fact, in Sweden, the number of all-cause deaths for those under 65 from mid-February through April was actually down slightly over the past few weeks. And Sweden didn’t implement a lockdown
wow. so far sweden's all cause deaths from mid feb to end of april (weeks 10-20) is actually below average for an… https://t.co/X2VVSSCW4B— el gato malo (@el gato malo) 1589918034.0
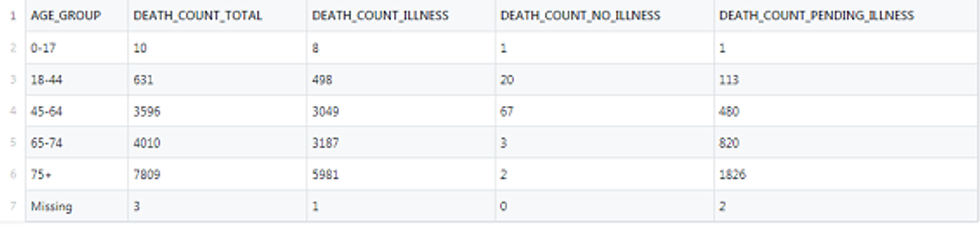
Also, almost all deaths are among those with known cardiovascular and neurological diseases or who had diabetes or other serious conditions grave enough to be placed on the death certificate. Even in New York City, only 0.6% of recorded deaths where comorbidities were confirmed did not have any existing comorbidities.
The overwhelming majority of those who are at risk are not in the workforce, and the majority of them are already somewhat “locked down” in senior care facilities. We could have shielded them much more effectively with a healthy economy and hospital system with staff and cash from performing other procedures. Yet rather than learn from this simple data, mayors are pre-emptively canceling all summer events and colleges are altering schedules even for the fall!
The refusal of our government and media to more broadly publicize this information, broken down by age group, is going to accelerate the disproportionate degree of panic. This has real consequences for many other patients who are too scared to seek medical care because they wrongly fear death by COVID-19 more than their existing dangerous illness.
In the coming days, the public will be utterly shocked by how deeply we were lied to about the underlying premise and threat assessment behind the lockdown.
Want to leave a tip?
We answer to you. Help keep our content free of advertisers and big tech censorship by leaving a tip today.
Want to join the conversation?
Already a subscriber?