Horowitz: The lies about vaccine efficacy are exposed, so Scotland stops publishing data

If the truth hurts your narrative, you must censor it. But what if your own information harms your own narrative? Well, then you stop publishing it.
For the past few months, Scotland has been publishing age-stratified case rates by vaccination status in a very well broken-down chart every Wednesday afternoon, similar to the way the U.K. published the data every Thursday. The common thread observed from these trends was that the unvaccinated had the lowest case rate, the double-vaccinated had even higher death and hospitalization rates, and the triple-jabbed gradually had increasingly higher case rates, which clearly doesn’t portend good news even for hospitalization and death in the long run. When people like me started using their data, we were lambasted by the “fact-checkers” paid for by Big Pharma. Now Scottish health officials announced they will not be publishing the data at all.
“Public Health Scotland will stop publishing data on covid deaths and hospitalisations by vaccination status — over concerns it is misrepresented by anti-vaxx campaigners,” reports the Glasgow Times.
The notice of change was published on page 29 of the latest, and evidently final, Wednesday report from Feb. 16. “PHS is aware of inappropriate use and misinterpretation of the data when taken in isolation without fully understanding the limitations described below,” they decried.
You mean like screenshotting their own charts?
Obviously, there can be confounding factors, but those factors actually cut both ways. However, at the end of the day, these are age-stratified adjusted case rates per 100,000 and are completely fair game to use. No vaccine that is anywhere near as effective as they make it out to be should be netting these results.
Here is the latest case rate chart from the final report:
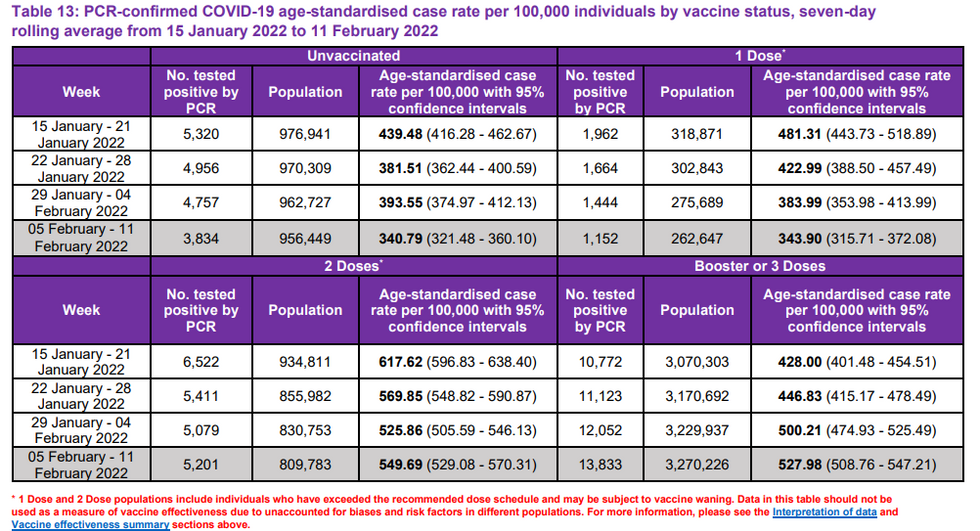
As you can see, for the past two weeks they have been placing disclaimers at the bottom of the charts.
What the chart clearly shows is what we have been seeing throughout the world — from the U.K., Canada, and Israel, for example — namely, that the second shot has gone negative a long time ago and the third shot is gradually following in the same direction. The public health officials themselves are demanding that people get boosters because they say the other shots wane. Well, logic would dictate that now that we are three to five months into the boosters in most places, they are waning as well. We also know that waning efficacy is potentially associated with a Trojan horse effect of antibody dependent disease enhancement, something the FDA admitted was never studied in the long run (at the time they thought the shots wouldn’t wane) but would be a risk “potentially associated with waning immunity.”
The main argument of those who are against us screenshotting their own charts to point out what they themselves have admitted is a speculative theory that perhaps the vaccinated test more often than the unvaccinated. That is a purely speculative confounding factor in the favor of the vaccine, but here is a concrete proven confounder against the vaccine: Scotland counts the first 21 days of the first vaccine as unvaccinated and the first 14 days of the third vaccine as double-vaccinated. We already know from Alberta’s data (which of course they also took down since we cited it) that roughly 40% of cases, 47.6% of hospitalizations, and 56% of deaths among the vaccinated occurred within 14 days of vaccination! So if anything, many of the cases and deaths ascribed to the unvaccinated are caused by the immune suppression of the first shot, and many cases and deaths ascribed to the double-vaccinated makes that cohort look even worse than it already is in order to ameliorate the image of the boosters.
Furthermore, if the higher case rates among the vaccinated are the result of a higher testing rate, then why would the double-vaxxed also be worse off than the unvaccinated for hospitalizations and deaths, as PHS has been showing for weeks in its other charts?
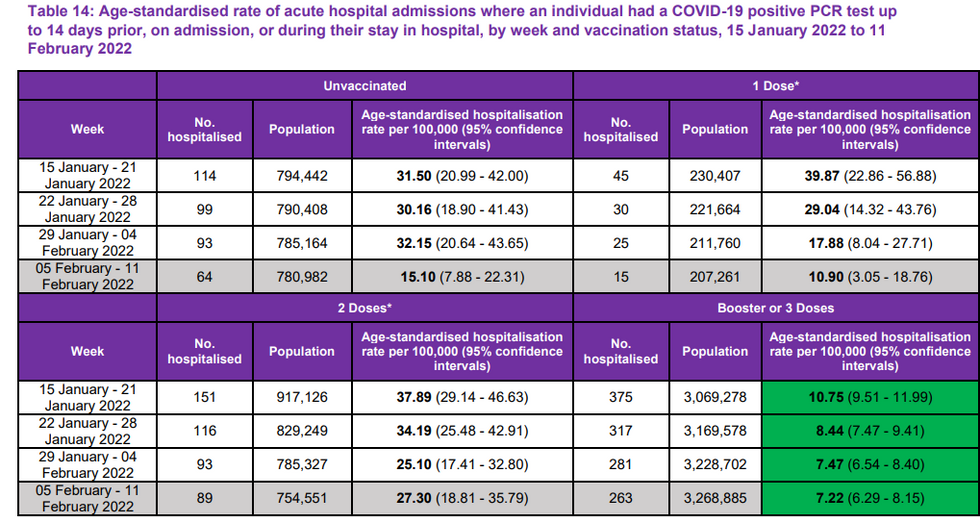
It’s quite evident that everyone is tested in the hospital. If anything, it stands to reason that the unvaccinated would be more aggressively tested even when admitted for other ailments and therefore potentially be roped into incidental hospitalization counts more often than the vaccinated. For example, in June 2021, Scripps Health in San Diego announced it would only test unvaccinated asymptomatic patients but not the vaccinated. Clearly, the testing requirements of the unvaccinated and the counting of the (immune-suppressed) partially vaccinated as unvaccinated would be confounding factors for woefully overestimating unvaccinated hospitalizations, not the other way around.
Also, why would the triple-vaxxed test less often than the double, who test more often than the single or unvaccinated? And why would the waning always continue in the same direction throughout the pandemic? As you can see from the U.K. Health Security Agency weekly reports, the efficacy of the shots constantly wanes with every new weekly report, a phenomenon that cannot be explained away by testing rates.
Infection rate growth (Rept Wks 50 to 7) since Omicron became dominant is much higher in all boosted cohorts. In boosted adults \u226550, growth increases sharply with age or time since boosting - whereas infection rate growth in the unvaxxed is more consistent across cohorts. Why?pic.twitter.com/DhQ2r9wlcz— Don Wolt (@Don Wolt) 1645113384
UKHSA COVID Hospitalization Update: 2/17/22\n\nWeek 7 report just came out.\n\nBefore and After % of Total Hosps by Age Group by Vax Status (dose).\n\nChart 1 - Week 6 Report\nChart 2 - Week 7 Report (current)\n\nIf anyone knows where to locate Pop Vax% by Age group, please show me.\n\n/1pic.twitter.com/ZXIVVfpCFp— Hold2 (@Hold2) 1645116891
Clearly, this picture points to dangerous waning efficacy that plagues every cohort within a few months.
The bottom line is that during the final week of reporting in Scotland, just 12% of the deaths are among the unvaccinated, and that is including the 21-day grace period of counting the single-jabbed as unvaccinated. Nobody is suggesting that there is no efficacy for some people for a period of time against serious illness before the shots wane. But to suggest that this is a pandemic of the unvaccinated, to ignore the negative efficacy on infection which has been true across the board since last summer, and to obfuscate the concern of waning efficacy on critical illness even as they themselves demand boosters defies willing suspension of disbelief.
Unbelievably, PHS admits that the shots first suppress the immune system before they ramp up antibodies. But instead of using this as a strike against the shots, they use that is a strike against the unvaccinated and assert that it is a factor for why you can’t even compare hospitalization or death rates. “Individuals who have not completed their vaccine schedule may be more susceptible to a severe outcome and could result in higher COVID-19 case, hospitalization and death rates in the first and second dose vaccine groups,” claims PHS in the report.
But if that is true, that is the fault of the manufacturers who made a shot that first makes you vulnerable during an ongoing pandemic. It’s one thing to have a shot that makes you more vulnerable for a few weeks during the off-season of a virus. But to do so during the pandemic is akin to telling someone in a foxhole during a firefight that they will be safer in a bunker 100 yards ahead but must first run across the field to get there. The risk of making that run should be counted against the bunker option, not the foxhole.
In other words, as I wrote in my original piece on the Scottish data that was “fact-checked,” “You have to look in totality where we are headed rather than manipulating a snapshot of time.” You can’t just pull out one period of time of some efficacy for some people. You need to consider the following:
- Vaccine injuries short term and long term, known and unknown;
- Other safer treatment options for COVID itself;
- A leaky vaccine that wanes in efficacy and runs the risk of enhancing the virus itself even while offering temporary protection for some;
- The cost to the immune system of constantly boosting people to deal with the abovementioned concern of waning efficacy and enhancement.
The bottom line is that the social media guardians are looking at a snapshot of time. If they were to study the trajectory and progression of the virus and the vaccine throughout the year, they would recognize an unmistakable pattern of waning and then negative immunity. A large study published in the New England Journal of Medicine by Weil Cornell Medicine-Qatar found (table 3) that the Pfizer vaccine waned very quickly after four months. By seven months, when adjusted for those in Qatar who already had prior infection, the Pfizer shot was -4% effective against transmission and just 44.1% effective against severe illness. Also, effectiveness against asymptomatic infection was -33% after seven months.
A Swedish preprint study in October 2021 looked at 1.6 million people in Sweden to examine infection rates and critical illness rates by vaccination status. They found a sliding scale of efficacy that wanes with time, but eventually turns negative. Here is a presentation of fully adjusted vaccine effectiveness against symptomatic infection for various demographics after 210 days:
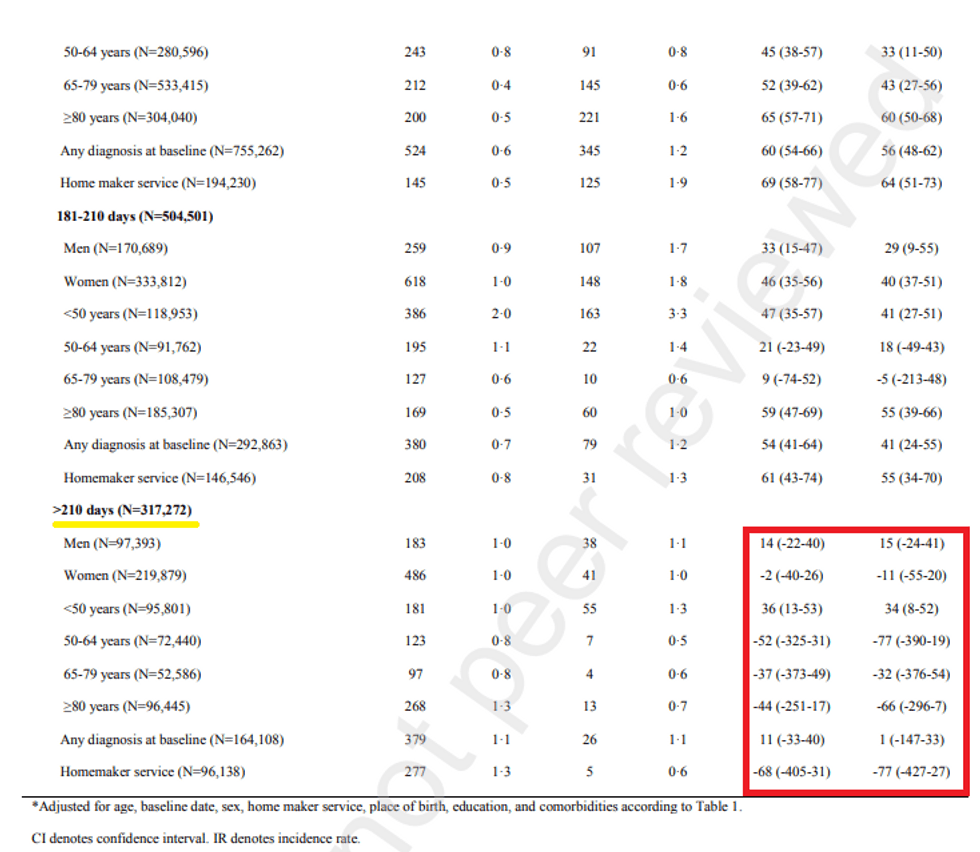
Clearly, it was known early on that the vaccine wanes and has the potential to go negative even with Delta, for which both natural infection and the vaccines offered better immunity. It stands to reason that this is certainly the case with Omicron, making it abundantly clear that the negative efficacy rate has more to do with potential Trojan horse antibodies than it does with vaccination-status bias of testing rates.
So what’s the solution? Go for a fourth and fifth shot? This week, Israeli researchers published a preprint study on the efficacy of the fourth shot, which found that after just one month, Pfizer’s shot is down to 30% efficacy and Moderna is down to 11%. At the same time, “Local and systemic adverse reactions were reported in 80% and 40%, respectively.” They conclude, “Low efficacy in preventing mild or asymptomatic Omicron infections and the infectious potential of breakthrough cases raise the urgency of next generation vaccine development.”
Remember, the FDA's industry guidance for EUA status (p. 13) requires a 50% threshold of efficacy to even get emergency use authorization, much less full approval!
Thus, who is actually misreading or inappropriately using data here?
The Israeli study also concluded that “most of these infected HCW [health care workers] were potentially infectious, with relatively high viral loads. Thus, the major objective for vaccinating HCW was not achieved.” Full stop. The biggest public policy debate is over the fact that somehow you not getting the shot affects other people. Here we see that even people with four shots were still infectious with high viral loads. To what degree the shot offers some degree of protection from serious illness for some people for some period of time should be a decision left to the people. Perhaps other people would like to choose therapeutics that offer protection that don’t run the risk of severe adverse reactions. But none of that should have bearings on another human being, and none of that should justify human rights violations.