Horowitz: Where are the governors? Now the feds will experiment with failed shots on our young children

It is undeniable that this vaccine is the quickest-waning and deadliest one in history. Even if one believes that for older adults the cost-benefit analysis is still favorable — a determination hard to make with obfuscated data — it is incontrovertibly clear that young children don't need a vaccine for this virus, much less one that is known to cause myocarditis and numerous thrombotic ailments.
Just consider the fact that in Michigan alone, 574 vaccinated people died of COVID (not including those half vaccinated who are most vulnerable), more than the number of children who died nationally all year. And that factors in the likelihood that a significant number of those children didn't die from the virus itself.
See those two numbers:574 vaccinated people died with Coronavirus in Michigan just this year. It’s state data; no… https://t.co/YxwsPFgH33
— Yossi Gestetner (@YossiGestetner) 1634775923.0
The Nuremberg Code dictates, "The degree of risk to be taken should never exceed that determined by the humanitarian importance of the problem to be solved by the experiment." Yet not only will the shots be approved within the next two weeks, they will be immediately forced upon children through a carrot-and-stick approach and eventually through mandates. California has already mandated them in school the minute they are approved for experimental emergency use.
The AP reported Wednesday that "within hours" of formal approval of the Pfizer shot for children 5-11 by the Centers for Disease Control and Prevention advisory panel, which is scheduled to meet on Nov. 2, "doses will begin shipping to providers across the country, along with smaller needles necessary for injecting young kids, and within days will be ready to go into the arms of kids on a wide scale."
This is as shocking and demonic as it is illogical. Yet they want to cover up the debate as quickly as possible and make this a reality in a shock-and-awe campaign. Their swift obsession with putting this in the arms of children after it has failed to even protect the elderly now raises even more suspicion about the entire premise of using this shot on anyone. Why would even the most pro-COVID-shot lobbyist ever have the least desire to use something like this on children, considering the myocarditis concerns alone? And unlike other approved shots, this one will be forced upon children with a degree of vigor never seen before.
It's no longer enough for Republican governors to merely pretend to oppose mandates, while still suggesting these are the safest and most effective shots ever. It's time for them to learn from the past nine months. We now have so much real-life experience with this shot. Just consider some of the following information we've learned:
- There are now 16,766 deaths logged into VAERS, as well as nearly 70,000 hospitalizations. We already know from previous studies that VAERS only captures 1% of adverse events, and no other shot has come with such a stigma against reporting it for harm, often at the threat of the physician losing his job. Medicare data seems to hint to a much broader cohort of vaccine casualties. Yet rather than further study these unprecedented events, they are rushing to inject children who don't need the shots anyway and for whom the Pfizer shot in particular will only offer a few months' protection (if that, given the changing variants).
- It would be one thing if the shots actually worked and COVID was basically in the rearview mirror, so we would decide to have children piggyback on the great success of the vaccine for adults. Instead, the virus is circulating more prolifically than ever before, the top five states for COVID spread are now among the most vaccinated states in the country, and countries with high vaccination rates like England are now following Israel's footsteps in experiencing the most deadly wave to date. Again, why are we not first investigating whether the suboptimal antibodies produced by the vaccine are not in fact making the virus worse, as top vaccinologists like Geert Vanden Bossche and Luc Montagnier warned, rather than pushing it on young children who are not in danger from this virus? Why are governors and legislators not calling in scientists like Dr. Ryan Cole to hear their concerns that the leaky vaccine is creating a super-infection and that more boosters and shots for younger people with a vaccine concoction that is already outdated will make the virus more virulent?
Sadly, the more we vaccinate with a defective shot in middle of a pandemic, the more we risk eventually raising the virulence level of the virus to the point that, in the irony of all ironies, it might someday clinically affect young kids.Antibody-dependent enhancement https://t.co/rrWhlM8xvv
— Wittgenstein (@Kukicat7) 1634668993.0 - Wenow know that the spike protein no longer stays in the shoulder muscle and evengoes throughout your bloodstream. A newpaper was published in the Journal of Immunology by researchers fromSt. Joseph's Hospital in Phoenix and the Yale Department of Pathology showingthat the Pfizer shot causes "circulating exosomes with SARS-CoV-2 spikeprotein" to travel through the bloodstream and, in their estimation, only wanefour months later. Already in February, astudy published in the Frontiers in Molecular Biosciences concluded,"Our findings indicate circulating exosomes' significant contribution toseveral processes—such as inflammation, coagulation, andimmunomodulation—during SARS-CoV-2 infection." In other words, the virus itselfspreads because the pathogenic spike is carried by exosomes, which are tinybiovesicles released into surrounding body fluids. How does this not indicatethat the spike from the shot travels throughout the body and into fluids andspreads to others much the same way the virus itself does? Could that explainthe aggressive turbocharging of the "virus" after the mass vaccination? Remember,Pfizer's own trial protocol seemed to indicate that it can spread through skin-to-skin contact in "inhalation."
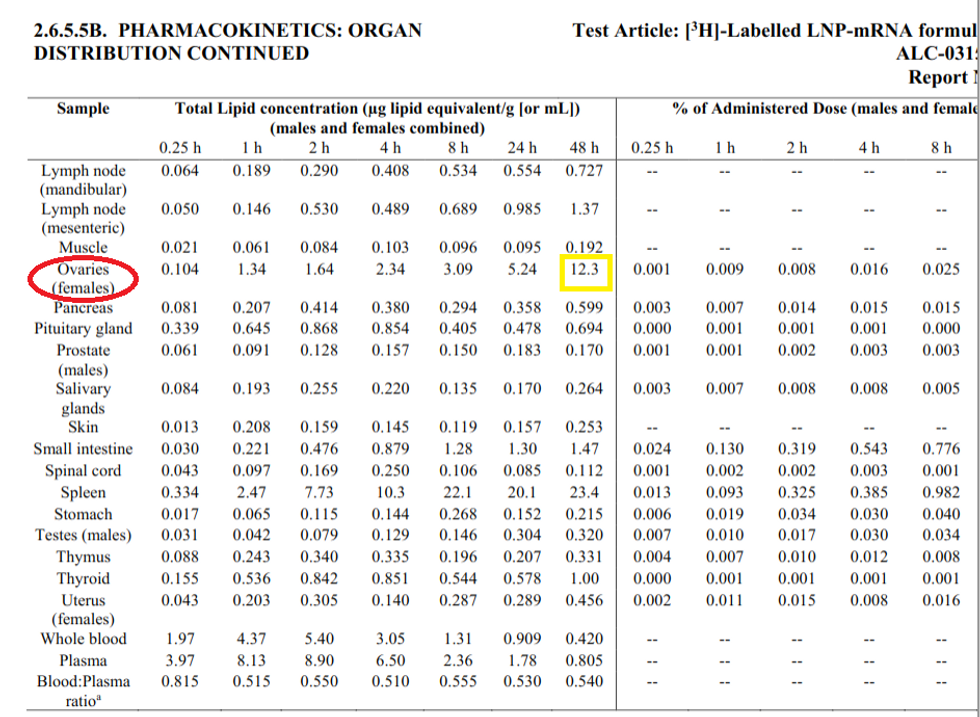
- Whatcould be some of the possible ramifications of the spike spreading throughoutthe body aside from blood disorders? How about fertility issues? A shocking newpreprint study authored by researchers from Washington University inSt. Louis, the University of Illinois at Urbana-Champaign, and Harvard found ashockingly large number of women experienced menstrual irregularities from theshots. They found 42% of women experienced heavier bleeding, while only 44%reported no changes to their menstrual cycles. A whopping 66% ofpost-menopausal women experienced breakthrough bleeding. A University of Chicago survey sought torecruit 500 women with menstrual irregularities in order to study the cause andeffect, and instead, they got 140,000 submissions. Could this be because, as a biodistribution report in Pfizer'spharmacokinetic pre-clinical animal study submitted to the Japanesegovernment found, the lipid nanoparticles of the vaccine were accumulating inthe ovaries in significant numbers – more than in any other place but thespleen?
- The unfavorable cost-benefit analysis is perfectly evidenced in a new Israeli 29-day follow-up study of 12- to 18-year-old vaccinated children. The study published in the New England Journal of Medicine found ZERO deaths and severe illness BOTH in the vaccinated and in the control (unvaccinated) groups.
The entire benefit of the shot was merely a decreased likelihood of getting infected with minor illness for a very short period of time. Keep in mind that numerous studies have shown that those who get the shots are initially more susceptible to getting the virus from the time of the first shot until 14 days after the second shot. As such, we are trading a narrow time frame of decreased likelihood of mild infection for a lifetime of known and unknown side effects for a cohort that does not get clinically ill from this ailment to begin with. Now they want to take this show down the road to the younger children too. Ironically, with the virus circulating so prolifically, most of these children will wind up becoming more likely to get the virus before they even reach the window of “benefit" from the shots. And that's assuming they haven't worn off even further with the ever-mutating virus. We are offering young children the equivalent of last year's flu shot, through a novel mechanism that is infinitely more dangerous.12-18 years old, 29 days "surveillance" after vaccination.Adverse events? -Not included.All-cause hospitalization… https://t.co/2wZ3GsZBA4
— Ran Israeli (@RanIsraeli) 1634802747.0
Thus, it's no longer enough for governors to simply praise the shots categorically and have their respective health departments promote them like candy, while stopping short of a mandate. It's time for them to implement a full investigative and regulatory regime that we used to count on the FDA for before they were bought out by Pfizer. The lack of oversight has gotten so bad that the CDC is now allowing the complete destruction of the scientific method and greenlighting the "mixing and matching" of different shots and boosters without any safety data. They want people to get all kinds of shots, as many as they want, and whomever. Facts and safety don't matter. It's become a cult. The state governments need to ask all the questions being ignored by the feds and refuse to endorse these shots for anyone, much less kids, until they are answered.

