![]()
“The vaccines are incredibly safe. They protect us against Omicron; they protect us against Delta; they protect us against COVID." Those were the words of fully vaccinated CDC Director Rochelle Walensky while testifying before the Senate Health Committee with two masks on her face on Jan. 11.
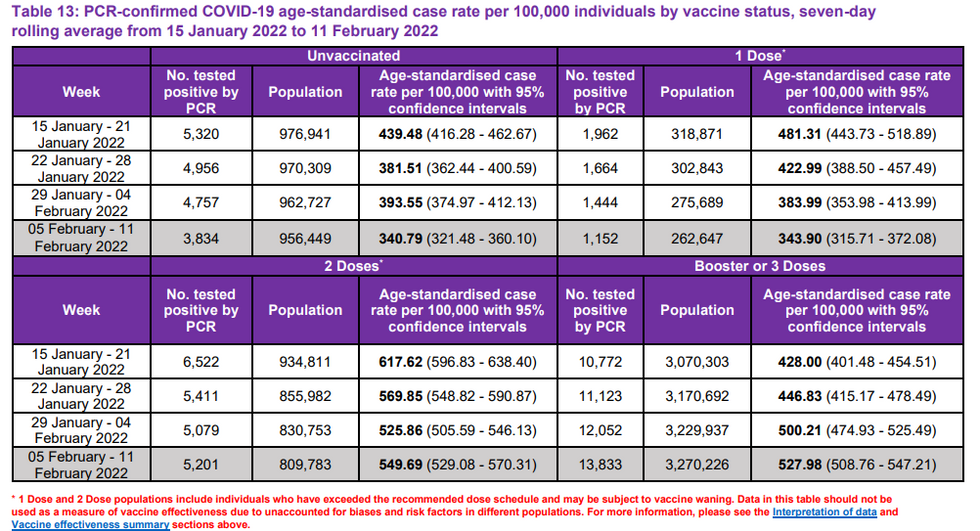
Scottish data shows that the COVID-19 age-standardized case rate is highest among the two-dose vaccinated and lowest among unvaccinated! It further shows this trend of negative efficacy for the double-vaccinated persisting for hospitalizations and deaths. Something is very wrong here, and together with other data points, it raises concerning questions about the negative effect of waning antibodies, constant boosting, and the consequences of a leaky vaccine with narrow-spectrum suboptimal antibodies against an ever-evolving virus.
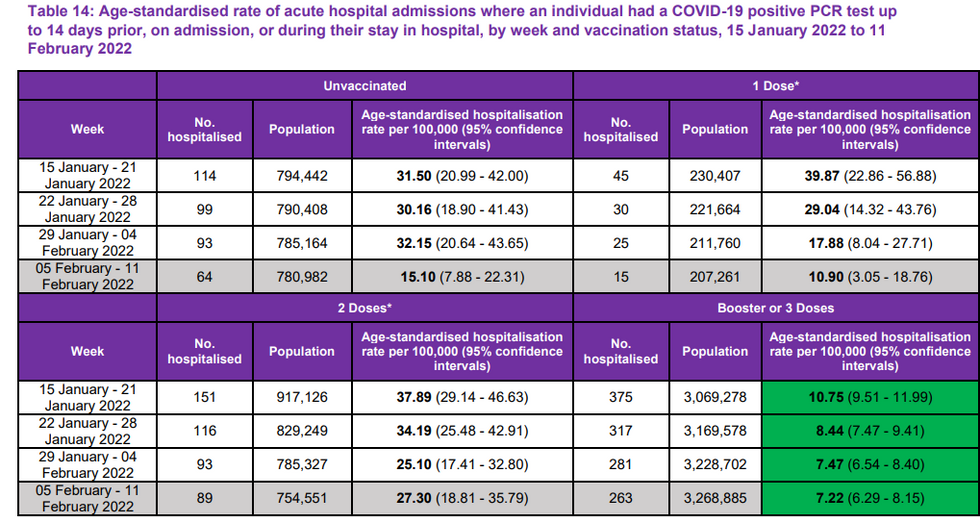
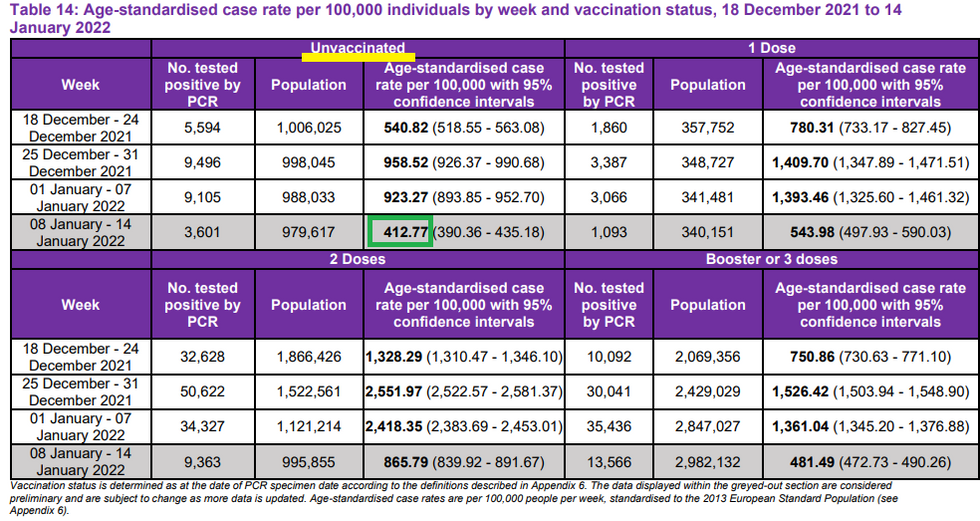
Every Wednesday, Public Health Scotland (PHS) has been publishing a weekly report on COVID data juxtaposed to vaccination rates. Table 14 of this week’s “Public Health Scotland COVID-19 & Winter Statistical Report” lays bare in plain English (and math) a rate of negative efficacy for the vaccine:
![]()
As you can see, while the overall Omicron wave seems to be receding in Scotland, age-standardized case rates per 100,000 people were the lowest in the unvaccinated cohort every week for the past four weeks. Thus, it’s not just the fact that the unvaccinated accounted for only 11.5% of cases the past two weeks, but even adjusted for age-stratified vaccination rates (PHS already does the math for you) the unvaccinated had the lowest infection rate out of the four cohorts – especially during the peak of Omicron. Furthermore, we see that even the triple-vaccinated clearly have no efficacy against infection, although they have some degree less negative efficacy than the double-vaccinated.
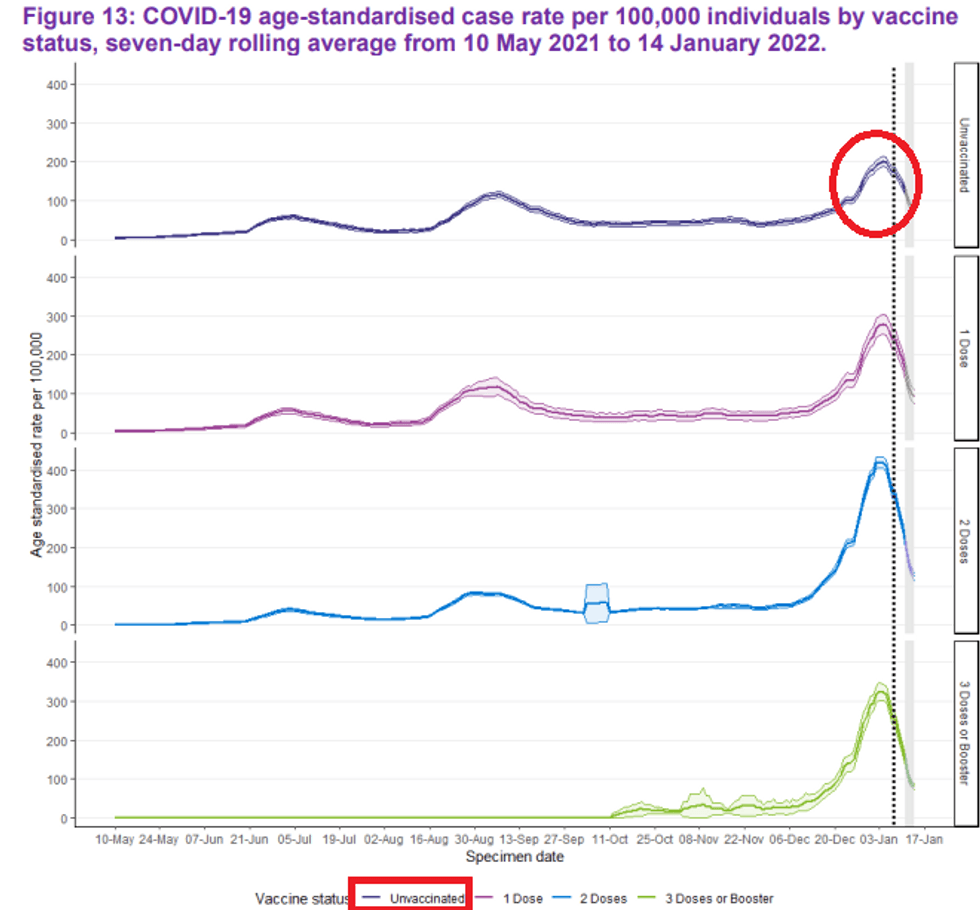
Here is a linear presentation of the depth of the Omicron wave by vaccination status, where you can see that the unvaccinated had the shallowest wave:
![]()
This also coincides with the latest data from the U.K. Health Security Agency of the entire United Kingdom. This data now shows higher rates of infection among the triple-vaccinated in all but the youngest people.
Triple-Jabbed Over-30s Have Higher Infection Rates Than the Unvaccinated, UKHSA Data Show https://dailysceptic.org/2022/01/20/triple-jabbed-over-30s-have-higher-infection-rates-than-the-unvaccinated-ukhsa-data-show/\u00a0\u2026pic.twitter.com/z5TnXT0sA7
— Andrew Bostom, MD, MS (@Andrew Bostom, MD, MS) 1642700314
Full stop right here. Any public policy measure – from vaccine passports to discrimination – cannot be justified under the science, even if one’s conscience is OK with apartheid. In fact, clearly this shows that, especially with Omicron, the vaccinated are the super-spreaders. Before we get to hospitalizations and deaths, the notion that the unvaccinated are somehow responsible for the continued spread of this virus is completely contradicted by the data. Some might suggest without evidence that the unvaccinated possibly have a higher rate of prior infection; however, Omicron seems to attack even those who already had previous versions of SARS-CoV-2.
Now onto hospitalizations and deaths. While the vaccines clearly provided some degree of protection for some people for several months against severe illness (while possibly causing even more spread), the Scottish data paints a concerning picture of the long-term consequences of the mass vaccination. People like Dr. Geert Vanden Bossche have been warning that if you mass-vaccinate with a leaky, narrow-spectrum (only recognizes spike protein) vaccine in middle of a raging pandemic, the virus would get more virulent over time.
This concern manifests itself at two time periods when the antibodies are “sub-optimal.” There is a period of a few weeks after the jab when the antibodies are strong enough to bind but not strong enough to neutralize, and then at the back end (estimated at four to six months for the original shot, but likely much shorter for the booster), a period when they wane. The media and public health tyrants like to focus your attention on a snapshot of time, but ignore the totality of circumstances that the shots are creating negative efficacy before and after, while using accounting gimmicks to mask the problem.
Remember how the lockdowns were hailed as a success for a number of countries that initially did well, while Sweden now has the lowest rate of excess mortality in Europe in 2021?
\u201cSweden now has a lower death rate than countries that went down the full lockdown route, including the UK, France, Spain and Italy\u2026 Economic recovery has been brisk\u2026 Sweden has not caused damage to the life chances of its children.\u201dhttps://www.theguardian.com/business/2022/jan/02/a-wounded-pm-and-ailing-economy-forces-england-to-go-swedish-on-covid?CMP=Share_iOSApp_Other\u00a0\u2026
— Prof. Freedom (@Prof. Freedom) 1641237709
Just as with lockdowns, the mass vaccination needs to be judged after all nine innings of the ballgame.
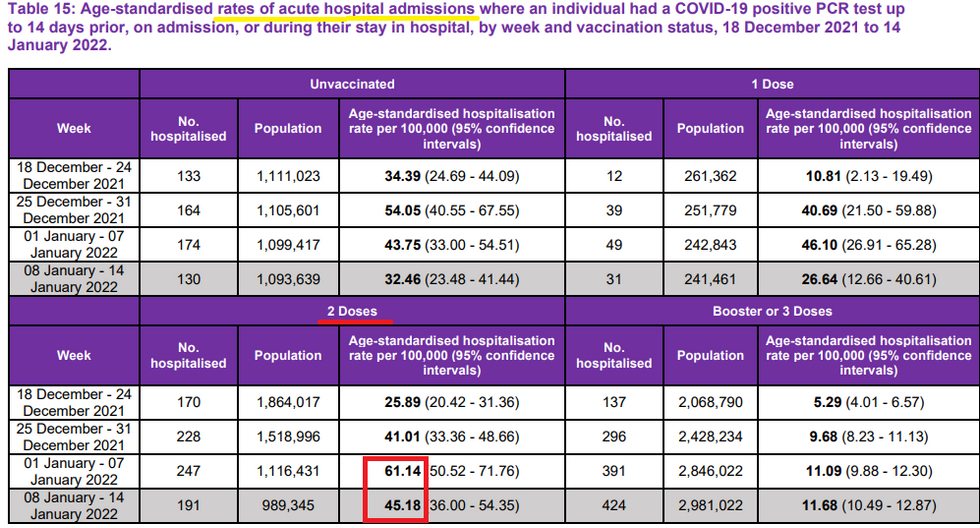
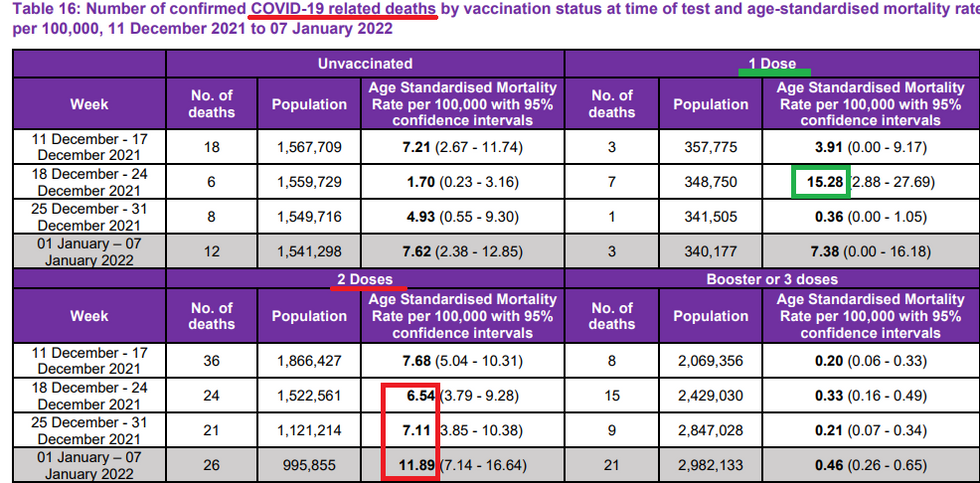
With that said, let’s take a look at tables 15 and 16 – the acute COVID hospitalization and death rates, respectively:
![]()
![]()
What is clearly evident both from the hospitalizations and deaths is that the double-vaccinated are now worse off per capita even against critical illness, and that pattern appears to be accelerating. Again, this evidently shows a pattern of negative efficacy even against critical illness over time as the shots wear off, increasingly quickly with Omicron. Why is there no desire to study the source of this negative efficacy and whether the fact that the vaccine is non-sterilizing, wanes quickly with sub-optimal antibodies, is narrow-spectrum, and is increasingly out of synch with the changing virus is going to make the pandemic worse in the long run?
Some will look at the chart and conclude that the boosters are amazing. But first it’s important to recognize that even the boosters don’t stop transmission at all even in the short run, and then, based on the latest hospitalization data, appear to wane just like the original shots. Relatedly, you will notice a pattern: the unvaccinated and two-dose cohorts always appear worse and the one-shot and three-shot cohorts always appear better. This is where the most important part of the data set comes into play.
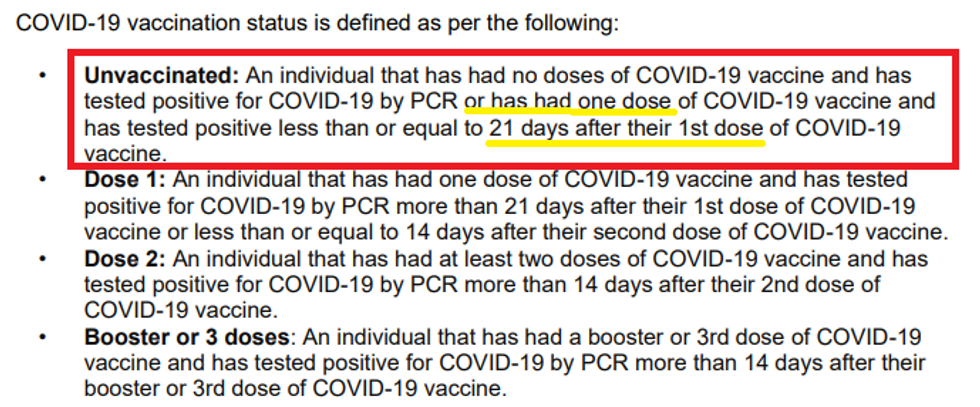
You see, all cases during the first 21 days after the first shot are counted in the “unvaccinated” cohort, while the first 14 days after one receives the 3rd shot is counted among the two-dose cohort. See the definitions from Appendix 6 of the report.
![]()
We know from numerous studies (see here and here) that people are actually the most vulnerable to COVID during the first few weeks on the upswing of the antibodies, when T cells are likely suppressed. This is why the health departments smartly count them in the unvaccinated pile. Hence, for all these months, all the cases and deaths from those made more vulnerable from the first shot – which is caused by the mass vaccination, not the unvaccinated – are counted against the unvaccinated. Over time, as the shots waned on the back end, the truth became evident. Now they are starting the cycle all over again by making the two-dose group look even worse than they are by dumping all of the cases caused by the initial take-up from the third dose into the cohort of double-vaccinated.
It’s the ultimate pandemic Ponzi scheme. Just wait another two months and see what the fourth-shot group looks like relative to the triple-dosers, as the immediate vaccination causes an even greater spike in cases. In other words, you have to look in totality where we are headed rather than manipulating a snapshot of time.
What this report shows is that just 18.5% of the hospitalizations in Scotland were unvaccinated, but even that number includes numerous people within 21 days of the first shot, which is clearly a very vulnerable time. It’s akin to telling someone in a foxhole to run across the field of fire to get to a bunker that might be safer, but he runs an even higher risk of getting cut down before reaching the bunker. Then, after a few hours, the bunker will get overrun by the enemy and you have to run through a new field of fire to get to the next bunker.
Likewise, when a therapeutic lowers symptom severity through immune suppression, it’s a flash in the pan. Eventually, that mechanism of action will come back to bite you in the proverbial arm. And this is even before we get to the long-term concern that multiple shots will create permanent immune suppression by creating original antigenic sin, a position now articulated by the European Medicines Agency and top Israeli immunologists.
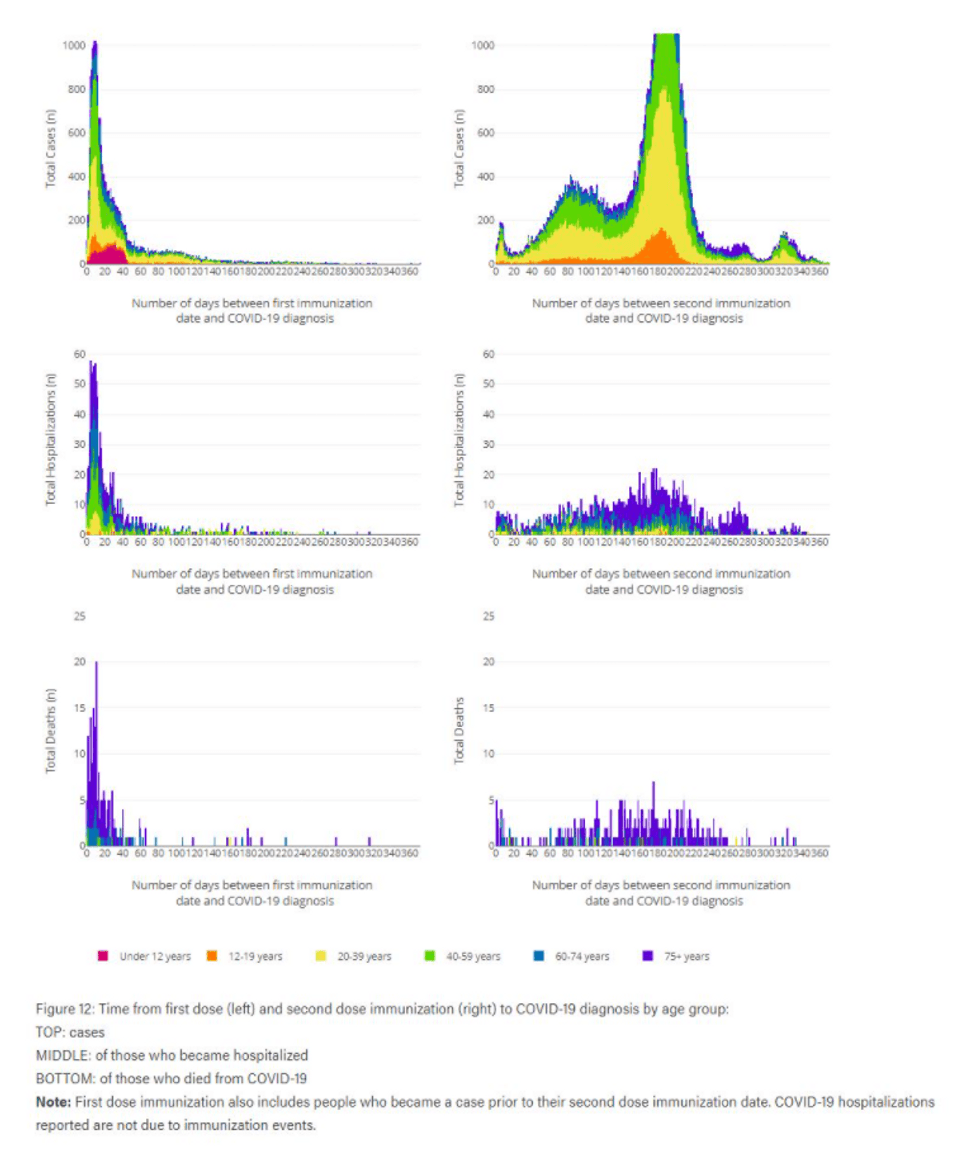
Just how prominent is the infection rate within the first 14-21 days of getting the shot, thereby completely distorting the epidemiological data and ultimate perception of efficacy of the shots? Although we don’t have data from the U.K. or U.S. on the timing of infection relative to vaccination period, Alberta, Canada evidently publishes some of that data. According to U.K. researcher Joel Smalley, who screenshotted the chart from the Alberta government’s website before it was taken down, roughly 40% of cases, 47.6% of hospitalizations, and 56% of deaths among the vaccinated occurred within 14 days of vaccination! Here is the graphical presentation that was on the website, according to Smalley. The top chart represents cases, the middle is hospitalizations, and the bottom is deaths:
![]()
Alberta, like many governments, counts the first 14 days as unvaccinated. In Scotland, they are counting the first 21 days after the first dose as unvaccinated and 14 days following subsequent doses in the cohort of the previous numbered dose. Obviously, we can’t mix the Alberta time-based data with the overall Scottish data, but common sense dictates that a bunch of cases from the immune suppression period of the initial vaccination are being blamed on the unvaccinated, and the perception of the booster shots is also likely being ameliorated at the expense of the double-jabbed cohort. For example, in Alberta, it appears that roughly 60% of the hospitalizations in the vaxxed cohort got COVID within 21 days of the shot, which in Scotland, would all be counted as unvaccinated cases. Thus, they deliberately chose the cutoff date for designation of vax status after the inflection point where they see the most COVID cases post-vax!
This deep dive into the data from Scotland should serve as a Rosetta stone for the macro observations we have seen from day one. We are seeing the most vaccinated nations and states being hammered with more cases than ever in a way that defies anything we should expect to see from a safe and effective vaccine. Here are just a few of the many examples:
I mean. When you compare case rates and vax rates for the past 3 weeks you'd think that the line wouldn't look like this. But it does. That trend line should be going in the other direction.pic.twitter.com/85Wdgj9Z2b
— Justin Hart (@Justin Hart) 1641840740
JUST IN - Israel: Over 14,000 IDF personnel are currently infected with COVID. In addition, 9,732 personnel in quarantine (JPost)
— Disclose.tv (@Disclose.tv) 1642598226
Israel , the only quadruple-vaxxed country in the world (also using mask mandates and Covid passports), just broke global record for daily Covid cases pic.twitter.com/G1ZDuVG2Ru
— Dr. Eli David (@Dr. Eli David) 1642537647
With N95 mandates, vaccine passports and 2 months of a lockdown for unvaccinated people, cases in Austria have reached a new high\n\nIt\u2019s amazing how consistently and comprehensively COVID authoritarianism and The Science\u2122 fails & how uninterested media outlets are in covering itpic.twitter.com/O1ABBdOOOO
— IM (@IM) 1642530717
UK HSA data shows infection rate growth correlates with vaccination rate for age cohorts >50. The more highly vaxxed an age cohort is - whether fully vaxxed or boosted - the faster the infection rate growth. Infectn rate growth in the unvaxxed is fairly consistent across cohorts.pic.twitter.com/40l01thdtS
— Don Wolt (@Don Wolt) 1642360856
Quebec, in midst of draconian lockdown, (unlike Ontario) publishes new hospitalization data by age group, vax status https://msss.gouv.qc.ca/professionnels/statistiques/documents/covid19/COVID19_Qc_RapportINSPQ_HospitalisationsSelonStatutVaccinalEtAge.csv\u00a0\u2026 \n\nThese are real counts, neither "normalized" relative to population nor "adjusted" by Ontario Science Table (or CDC). What do you notice?pic.twitter.com/2Q5hPfxam0
— Stephen McIntyre (@Stephen McIntyre) 1642354931
Sigh...pic.twitter.com/zeVA6mtZSi
— Covid19Crusher (@Covid19Crusher) 1641995379
Omicron waves in Israel and South Africa, per capita.\n\nIsrael has given 4x more vaccine shots to its population than South Africa.\n\nYesterday, Israel was exhibiting the higher incidence per capita in the world among large countries.pic.twitter.com/tIryUthm6j
— Covid19Crusher (@Covid19Crusher) 1642778142
Dr. Fauci recently told Bloomberg news that “there are some inherent ‘non-believers’ that no matter what you say, they give you a real problem.” He’s right. It takes a true religious level of adherence – like a believer – to continue supporting his narrative, despite the plain facts before our every eyes.