Horowitz: The treatment nihilism of our government continues unabated

The calls have become all too familiar. People who know that I’m friends with a bunch of top-notch doctors who actually treat COVID call up desperately searching for someone who will help. Last week, I got a call from a family member of a 47-year-old diabetic who suffers from epilepsy and hypertension who was in a Maryland hospital on BiPAP with a blood oxygen level of 83. This man kept away from people for two years and got three shots, but they failed him, and now he was getting nothing but the dangerous remdesivir. Oh, and the monoclonal antibodies are not available. This man now suffers the fate of hundreds of thousands of other people who are victims of therapeutic nihilism.
Just how much does the federal government want to choke off all forms of outpatient treatment for COVID, despite the evidence of so many affective therapeutics? As they make the monoclonal antibody treatments scarcer by the day, the NIH has now manipulated its own website to cover up its original position on ivermectin.
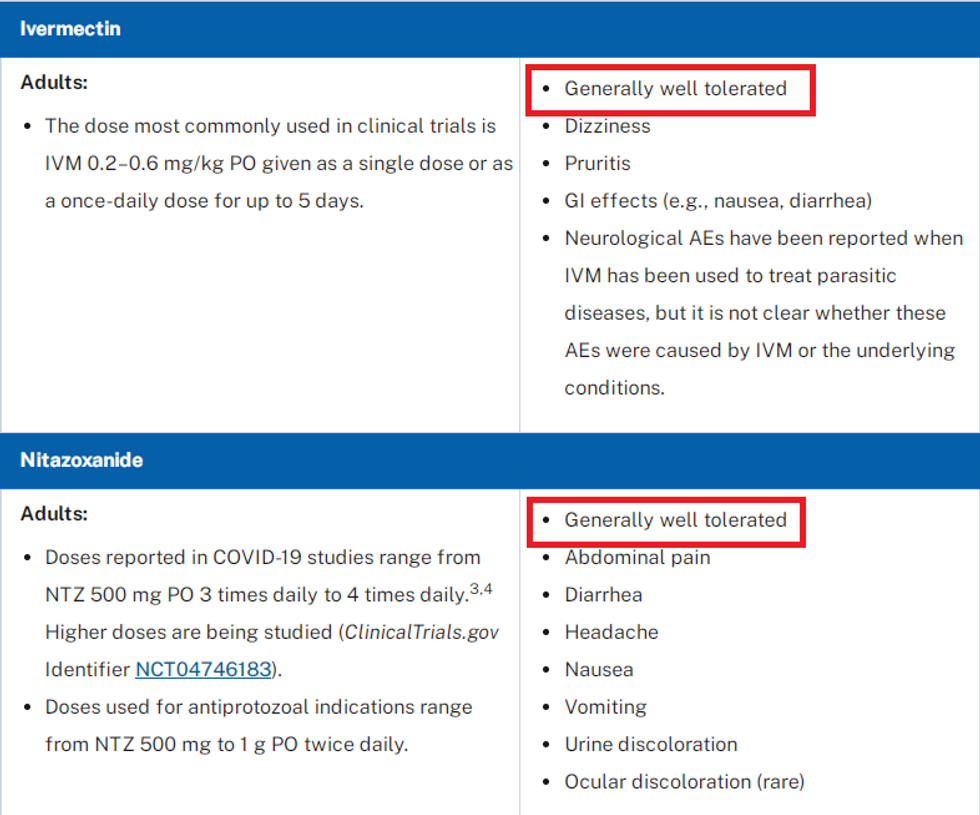
In October, I referred people to the NIH’s chart 2E, which placed ivermectin and nitazoxanide on the same footing as remdesivir in potential antiviral agents against COVID. At the time, I noted that while the NIH admitted in the chart that remdesivir (a big money-maker for hospitals) has the potential to cause kidney failure and liver toxicity, ivermectin and nitazoxanide were given the distinction of “generally well tolerated,” which is a term used to describe a near-perfect drug. I warned people to screenshot it (available on the Wayback Machine), lest the NIH remove or modify the page.
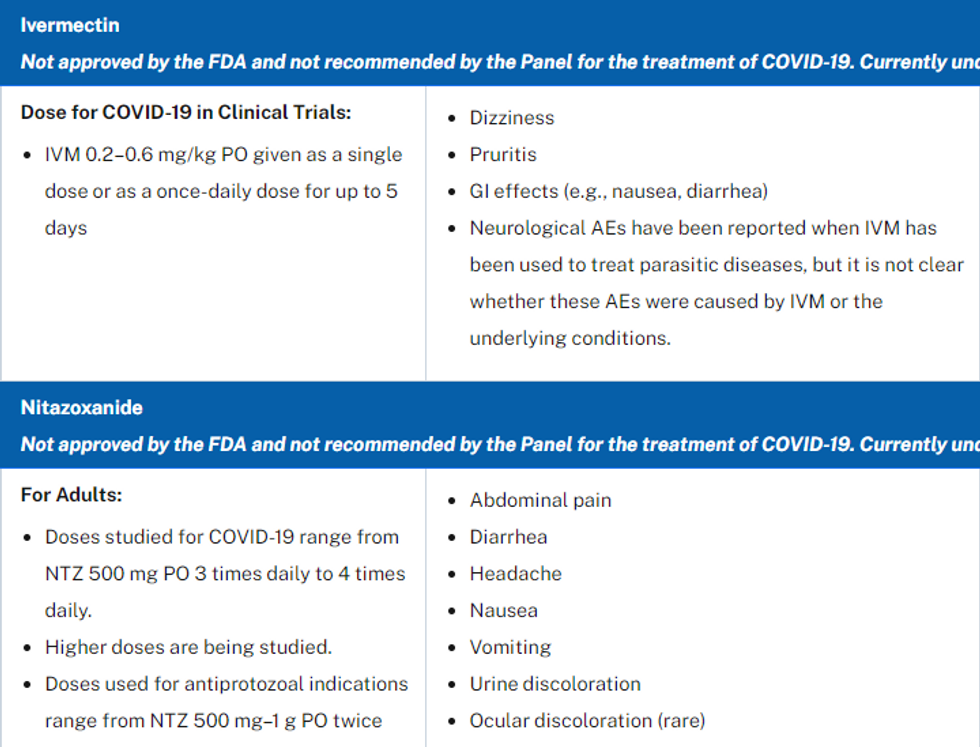
Well, it turns out that after many of us exposed the agency’s own position on ivermectin, it indeed removed the page, and instead, the URL takes you to an updated chart “2F” with changes. Updated on Dec. 16, the new chart specifically says that remdesivir is approved and the other two drugs are not. Additionally, it removes the status of “generally well tolerated” from ivermectin and nitazoxanide.
Here is a screenshot of the old 2E chart of side effects of ivermectin and nitazoxanide.
Now here is the updated version without the “generally well tolerated” status.
Remember, the original chart was updated on July 8, 2021, well into the pandemic. Nothing has changed since July other than ivermectin becoming mainstream in public knowledge. The approval status was the same then as it is now, and there is zero evidence of more side effects. In fact, millions of doses have been administered without incident, and certainly much more safely than remdesivir. Even if one were to suggest that the NIH is dinging ivermectin based on its own lies and rumors about people getting sick from overdosing on the horse paste (because government has made it hard to get the human pills), how could officials possibly take the distinction away from nitazoxanide? It’s too rare and expensive for people to use, and there is little evidence people used it, much less had adverse reactions to this very safe drug.
Keep in mind that remdesivir is not even a fully approved FDA drug, while the other two have been approved for years with stellar safety profiles. The market category for remdesivir is still listed on the FDA National Drug Code Directory as “Unapproved Drug Other” and shows end marketing dates of 9/20/23 and 8/31/22. Both nitazoxanide and ivermectin, on the other hand, are categorized as FDA-approved drugs.
Indeed, it would be quite illuminating to get hold of FOIA documents of correspondence leading up to these changes.
Just as with hydroxychloroquine in 2020, Big Pharma and the media-government complex waged a blood libel against a long-standing safe drug, as if somehow people were dropping dead from it when it was never observed in any prior data dating back decades. In September, New Mexico health officials claimed two people in the state died of ivermectin overdoses. We all knew at the time that it made no sense, but the damage was already done. Now TrialSiteNews reports that New Mexico Human Services Secretary Dr. David Scrase admitted in a Dec. 1 online press briefing that the two people indeed died of natural causes, according to the coroner.
“Now, Scrase has acknowledged that his repeated, what he called ‘offhand,’ assertions were groundless,” reports TrialSite. “Two deaths were not caused by ivermectin, a long-used generic drug that was emerging as a covid treatment. Instead, he said that the pair died because they ‘actually just delayed their care with covid.’”
The New York Times and many other large media outlets enthusiastically jumped on these false assertions, yet none of them have corrected the record. To this day, the government and media continue to conflate animal and human ivermectin, ironically driving more people into the animal version because they are illegally choking off the FDA-approved drug, which is listed among the WHO’s most essential medicines. All the while, none of these people or entities involved in the war on treatments seem to have a problem with remdesivir.
There is simply no satisfying answer as to why anyone in their right mind would think the cost-benefit analysis of remdesivir is better than ivermectin in any way. Also, when was the last time the government ever attacked doctors for prescribing a safe FDA-approved drug? Then again, this is not about ivermectin. Our government/media/pharma cabal opposes any and all cheap treatments for COVID the minute they become popular and refuse to even tell people to take aspirin to prevent blood clotting. In fact, they have already attacked aspirin, along with betadine nasal rinse, which has amazing data behind it.
Even if one somehow thinks that the 60+ ivermectin studies are not enough, fluvoxamine has solid data behind it from randomized controlled trials published in two of the top journals. A large, double-blinded randomized controlled trial published in the Lancet recently showed fluvoxamine reduced COVID-19 mortality rates by up to 91% and hospitalizations by two-thirds. A smaller clinical trial published in JAMA showed that zero COVID patients in the fluvoxamine group deteriorated during the course of treatment. Yet there is not the shadow of an intent by the federal government to even study this drug at a time when they concede both the shots and the monoclonal antibodies have waned. Florida is the only state that is promoting this as a treatment.
Dr. Brian Tyson, an urgent care doctor who has treated 7,000 COVID patients in Southern California, told me that pharmacies will give doctors trouble even over filling nebulized budesonide or antibiotics for COVID patients. “They are denying hydroxychloroquine, ivermectin, Singulair, budesonide, Zithromax, and colchicine because they claim that there is no indication for COVID-19,” said Tyson in an interview with TheBlaze.
The problem is that, especially with the monoclonal antibody supply dried up, there are no “approved” treatments and there haven’t been for nearly two years. However, as Tyson says, “COVID-19 is not the problem; the symptoms from COVID-19 are the problem, and we absolutely have ways of treating or pre-empting those symptoms.”
“By blocking these prescriptions, there is no way to prevent the cytokine storm that leads to respiratory failure,” warned Tyson. “Withholding these drugs without any alternatives available should be considered malpractice on the part of these pharmacies who illegally practice medicine. We are seeing inflammation, thrombosis, and secondary pneumonias that need to be treated, and having to fight with a pharmacy over FDA-approved drugs is negligence that leads to loss of life or needless hospitalizations.”
Indeed, the FDA itself has made it clear that prescribing off-label is most appropriate when there are no other treatments available. The FDA has given clear guidance that physicians can always prescribe off-label FDA-approved drugs "when they judge that it is medically appropriate for their patient." In fact, the FDA has made it clear that there is a particularly strong rationale for prescribing off-label if there is no "approved drug to treat your disease or medical condition."
Clearly, the goal was never to flatten the hospitalization curve. The politicians and the hospital administrators (if not the doctors on the floor) are enjoying full hospitals and the power and money they bring in. Everyone knows the best way to clear the hospitals is to treat early and outpatient, when the virus is much easier to control.
Tyson likes to point out that it’s not a matter of any one drug that’s a magic pill, but multi-drug therapy that makes early treatment close to 100% effective. “We started seeing inflammation, so we used anti-inflammatories,” Dr. Tyson explained in an interview last year. “We saw blood clots, so we used anti-coagulants. We saw patients having trouble breathing, so we used asthma medications. … It wasn’t just one drug. It was the art of what we see and how those patients responded to what we gave them.” This is why Dr. Tyson never lost a patient who came to him within the first week … out of 7,000. Why is nobody in power interested in discussing with him what he is doing right and trying to replicate it?
The utter insanity of the therapeutic nihilism was perhaps best summed up in a tweet Dr. Tyson wrote a few months ago before he was banned from Twitter. Yes, the doctor who likely treated more COVID patients than anyone in the country was banned from speaking. Here is how he summed up the pandemic:
If you see inflammation, use anti-inflammatories
If you see blood clots, treat blood clots
If you see pneumonia, treat pneumonia
If you see hypoxemia, treat hypoxemia
If you know it’s viral, use antivirals
If you do nothing, quit practicing!!!





