New study questions value of giving mRNA shots to children for 'short-lived' 26% 'protection,' while FDA and CDC double down on booster push
A new study out of Qatar has raised doubts about the efficacy of mRNA COVID-19 vaccines amid a concerted campaign by both the Food and Drug Administration and the Centers for Disease Control and Prevention under President Joe Biden to push bivalent booster shots on children. It turns out the COVID-19 boosters may be far more effective at generating profits for Pfizer and Moderna than they are at actually keeping children safe.
The rundown
Booster shots didn't appear to protect Pfizer chairman and CEO Albert Bourla, who tested positive for COVID-19 in September after having caught the virus the previous month. They also didn't protect CDC Director Rochelle Walensky, who took ill from the virus in October, one month after receiving her booster, or FDA Commissioner Robert Califf, who tested positive this week.
Despite concerns about their efficacy and whether they may exhaust patients' immune responses, the FDA authorized new COVID booster shots for people 12 years and older on Aug. 31 before testing them on humans.
The boosters, which had only been tested on eight mice, were touted as "bivalent," meaning they would target the original COVID-19 strain as well as new Omicron subvariants.
Paul Offit, the director of the Vaccine Education Center at the Children's Hospital of Philadelphia and a member of both the National Institutes of Health working group on vaccines and the FDA's Vaccines and Related Biological Products Advisory Committee, said in September that "there's not clear evidence of benefit" of the vaccine in healthy young people.
Offit told CNN: "What I fear is that they're going to say everybody should get it when in fact, the healthy young person really is unlikely to benefit from the booster dose, and so I hope they targeted more specifically, to those really who are most likely to benefit from this additional dose."
Months earlier, Florida Surgeon General Dr. Joseph Ladapo announced that healthy children shouldn't get the vaccines, as the benefits are dubious and the risks are potentially substantial.
The FDA clearly heeded neither Offit's nor Ladapo's warnings, because on Oct. 12, it authorized the bivalent boosters for children anyway. The CDC also authorized the bivalent booster shots for children the same day.
CDC Director Rochelle Walesnky said that an "updated vaccine can help bolster protection for our children this winter."
Fox News Digital reported that to be eligible for the new bivalent booster, children must first get two doses of the outdated vaccine, which, according to the New England Journal of Medicine, has "no effect against the omicron variant."
Extra to authorizing the shots, the FDA has mounted a pressure campaign to have parents get their children boosted.
FDA vaccines chief Peter Marks stressed in a video series on social media this month that giving kids over the age of 5 the booster will help them "avoid the worst outcomes of COVID-19."
Marks told the AP, "Right now is the time for people to consider going out and getting the updated" shot.
It turns out, however, that the mRNA shots may not just be woefully ineffective at protecting pharmaceutical executives and federal officials from COVID-19.
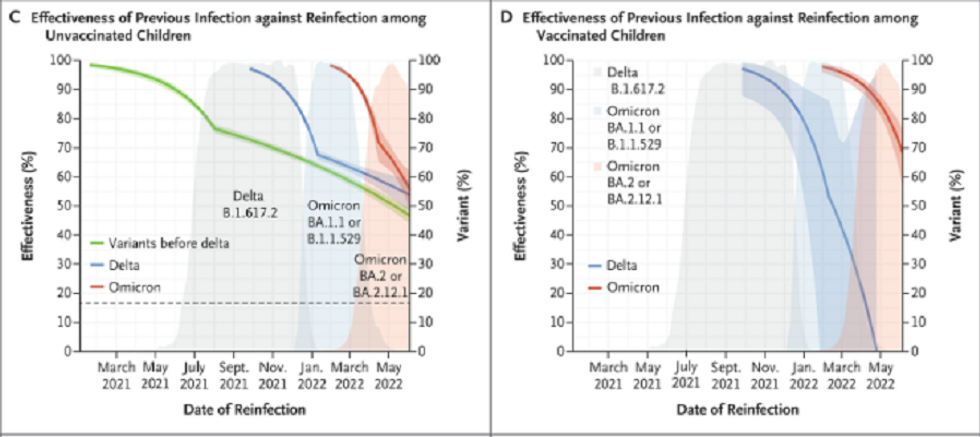
A new academic paper published Nov. 2 in the esteemed New England Journal of Medicine discussed the results of a Qatari study that tested the effectiveness of the primary Pfizer-BioNTech mRNA vaccine series in children with no previous record of infection.
Not only did the Pfizer vaccine's effectiveness drop precipitously in children after mere weeks, but it ultimately went negative for children ages 5 to 11.
The scientists' findings "suggest the need to reconsider the value and strategies of vaccinating healthy children in the omicron era."
The study
The paper, entitled "Covid-19 Vaccine Protection among Children and Adolescents in Qatar," indicated that the Pfizer vaccine series targeting children rapidly waned in effectiveness right after the second dose, going negative for some groups after just several weeks.
Its overall effectiveness was at best 25.7% averaged across ages 5-17: 46.3% among children ages 5 to 7; 16.6% among children ages 8 to 11; 35.6% among adolescents ages 12 to 14; and 20.9% among those 15 to 17 years of age.
Although those in the older cohorts had slightly longer "protection" because they had received larger doses, scientists nevertheless observed "rapidly waning protection."
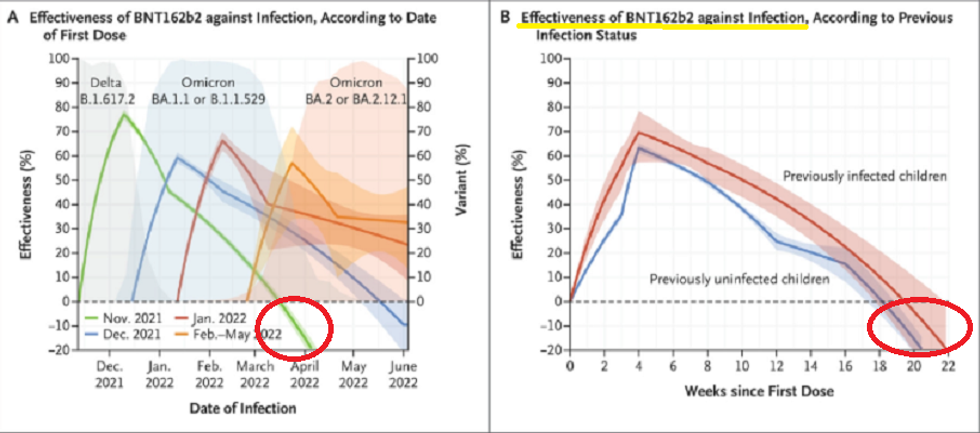
Referencing the data in the second graph from this study seen below (shared by Dr. Tracy Beth Høeg, an epidemiologist who advises Florida's Department of Health), Just the News reported that the lower confidence interval boundary for children ages 5-11 after two months and median after four months were both around -10, meaning the vaccinated kids were more likely to get infected.
Another dose
The Miami Herald reported that as of Nov. 3, over 22 million people in the U.S. had received the newest bivalent COVID-19 booster.
According to a new preprint study published Nov. 1 to medRxiv, which has yet to be peer-reviewed, those who received a third dose may have less protection against infection with the Omicron variant.
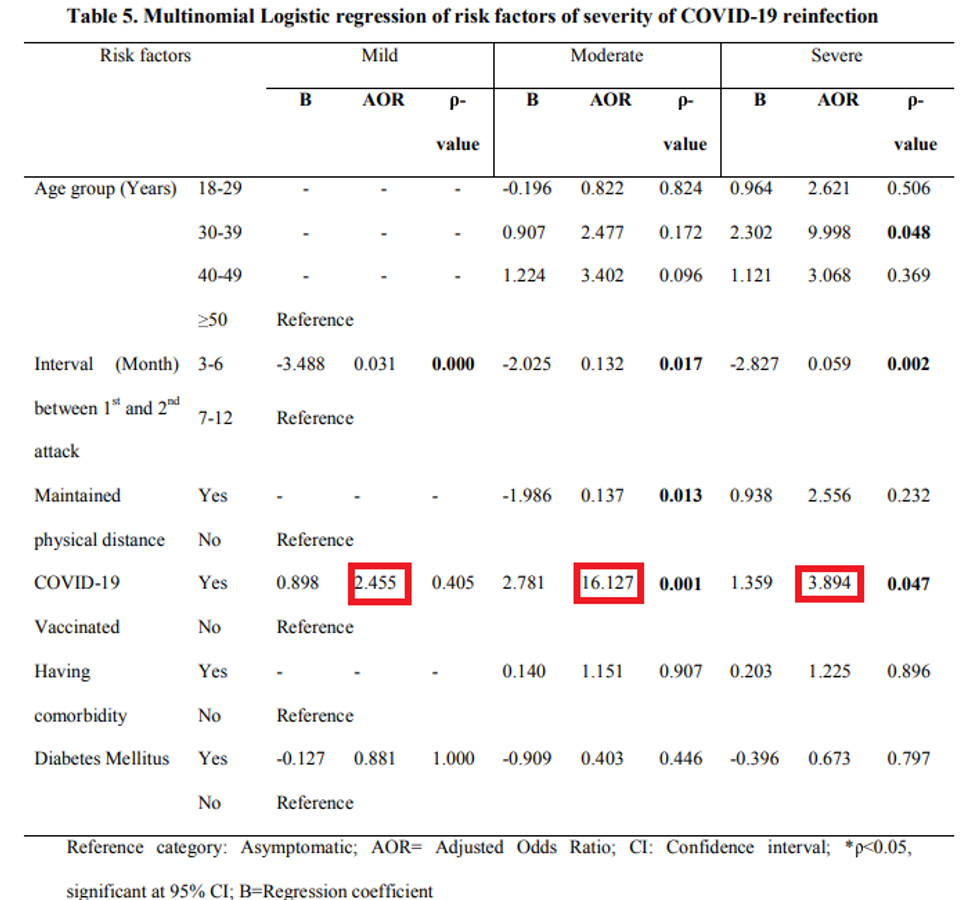
Dr. Daniele Focosi, a hematologist at Pisa University Hospital in Italy, wrote, "If you got infected with Omicron at any time, a third vaccine dose actually doubles your risk of reinfection compared to 2 doses only."
Just the News reported that while Pfizer CEO Albert Bourla claimed the bivalent booster prompted "increased neutralizing antibodies" that afforded the boosted "better protection" against Omicron subvariants BA.4/5, a Pfizer official admitted to the FDA that "there is no established correlate" between antibody levels and protection from disease.
Vinayak Prasad, a hematologist and professor of epidemiology and biostatics at the University of California, wrote on Substack that the government's "entire vaccine policy seems to be interested in giving Pfizer and Moderna a perpetual market share for a yearly vaccine. But seems to have no interest in generating credible randomized control trial evidence to inform the public. As such, they fail the American people."