Horowitz: New study shows more effective immunity from prior infection than in vaccinated among organ transplant recipients
Few people are as immunocompromised and vulnerable to COVID as solid organ transplant recipients (SOTRs). Those are the people whom the medical establishment suggests should get shots and boosters early and often — even if they have to "mix and match" different variations of the shots. However, given the fact that these people are also the most vulnerable to complications from the pathogenic spike protein of the shots, why are doctors not first making sure they don't have natural immunity? A new study demonstrates that it is criminal to assume the risks of vaccination for SOTRs with prior infection.
We already have at least 122 studies attesting to the durability of immunity from prior SARS-CoV-2 infection, many of which clearly show that immunity to be much stronger and longer-lasting than vaccine-mediated immunity. However, a new study from researchers at Ajmera Transplant Centre, University Health Network, in Toronto, Canada, demonstrates that even organ transplant patients have robust T cell immunity from prior infection, much greater than those who are vaccinated.
"Vaccinated SOTRs mounted significantly lower proportions of S-specific polyfunctional CD4 + T-cells after two doses, relative to unvaccinated SOTRs with prior COVID-19," concluded the authors of the study, published in the Journal of Infectious Diseases. "Together, these results suggest that SOTR generate robust T-cell responses following natural infection that correlate with disease severity but generate comparatively lower T-cell responses following mRNA vaccination."
Rather than studying the less meaningful antibody responses, the researchers studied T cell responses in three cohorts at Toronto's University Health Network (UHN) Transplant Centre: SOTRs who had prior infection but were not subsequently vaccinated, SOTRs who were vaccinated 4-6 weeks prior to the study but never had the virus, and a control group of regular non-SOTRs with prior COVID. While the non-immunocompromised naturally immune cohort obviously mounted the greatest T cell response, the study still found that SOTRs with prior immunity had robust antigen-specific helper (CD4) and killer (CD8) T cells. Overall, the researchers found a detectable antigen-specific T-cell response in SOTRs with prior immunity at a 41.4% greater frequency than in the vaccine-only group. Also, most of those in the vaccine cohort received the Moderna shot, which is believed to be more potent than the Pfizer shot.
The findings of this study are a bombshell, because they suggest, at least in the short run, that even the most immunocompromised people with prior infection mount a serious antigen-specific T cell response that, unlike the vaccines, targets the nucleocapsid and membrane of the virus, not just the spike protein. While there is no long-term follow up in this study of SOTRs, it is important to remember that there are endless studies showing long-term and likely lifetime immunity from prior infection in the general healthy population. At the same time, we already have numerous studies and the reality of the current hard data from fully vaccinated countries hit hard with a new spread that the vaccine-mediated immunity completely wears off even for healthy people after six months.
Moreover, studies have already shown that the immunity conveyed by the shots might be particularly short-lived for the immunocompromised. For example, a study from Puerto Rico's Department of Health recently found the shots to be 0% effective in those 85 years and older after 150-200 days after vaccination. A massive Swedish study of half the country's population showed "notable waning among men, older frail individuals, and individuals with comorbidities" after about six months.
The results of the SOTR study raise some serious questions:
- How can our government continue to ignore the power of natural immunity if it is this potent even in organ transplant recipients?
- How can we continue denying organ transplants to those who don't get the shot when some of them already had the virus and the shot itself doesn't work much?
- What is our solution to the immunocompromised? The shots barely work and will likely not work at all with the new variants, yet they are most dangerous to those people. They have never even been tested in people with kidney failure, much less an organ transplant. Are they supposed to live in their homes forever and atrophy with no safe and effective solution? Why is the government not studying the idea of using preventives like ivermectin, nitazoxanide, or monoclonal antibodies? A recent study of the general population showed that Regeneron given pre-emptively could work for at least eight months of protection without any of the severe risks that are associated with the failed shots. Our government won't even advise these people to use Betadine nasal spray after being around people.
Just how vociferously is our government working to deny natural immunity? At the other end of the health spectrum from elderly transplant patients are healthy children. As scandalous as it is to risk the shot on healthy kids, it's unfathomable to push the shot on kids who also had prior infection. Already in March, the government estimated that 42% of children 5-17 had prior infection, and that was long before the "Delta wave," which was more transmissible and seemed to infect kids more than the ancestral strain. We all assumed that a solid majority would have been infected by now and were waiting for new data to be published. But finally the CDC has updated its numbers, and you will never guess the new data. Immunity magically slid backward!
CDC finally updated their burden estimates... and they bizarrely find that the percent of age 0 to 17 ever-infected fell from 36.7% through May to just 29.9% through September.\n\nEven more bizarre: they claim a higher % of symptomatic COVID than infection. Literally impossible.pic.twitter.com/B3ujqf5Csw
— Phil Kerpen (@kerpen) 1636496130
Although they don't have new numbers isolated for 5- to 17-year-olds (excluding really young kids and babies who were generally more isolated), their numbers for the 0-17 cohort have slid backward from 36.7% through May to just 29.9% through September ... after Delta! This makes no sense because the media and our government were panicking about this wave hitting the schools much harder. For those with children in schools, we can attest to that fact that last year barely any kids got the virus, whereas this year more seemed to get it (although still mildly) and, unlike before, even spread it in the classrooms to some degree. There is simply no way that a majority of children are not already immune.
This is yet another example of the government retracting a talking point, data point, or study once our side begins using it.
What will it take for people to wake up and realize we are being lied to?






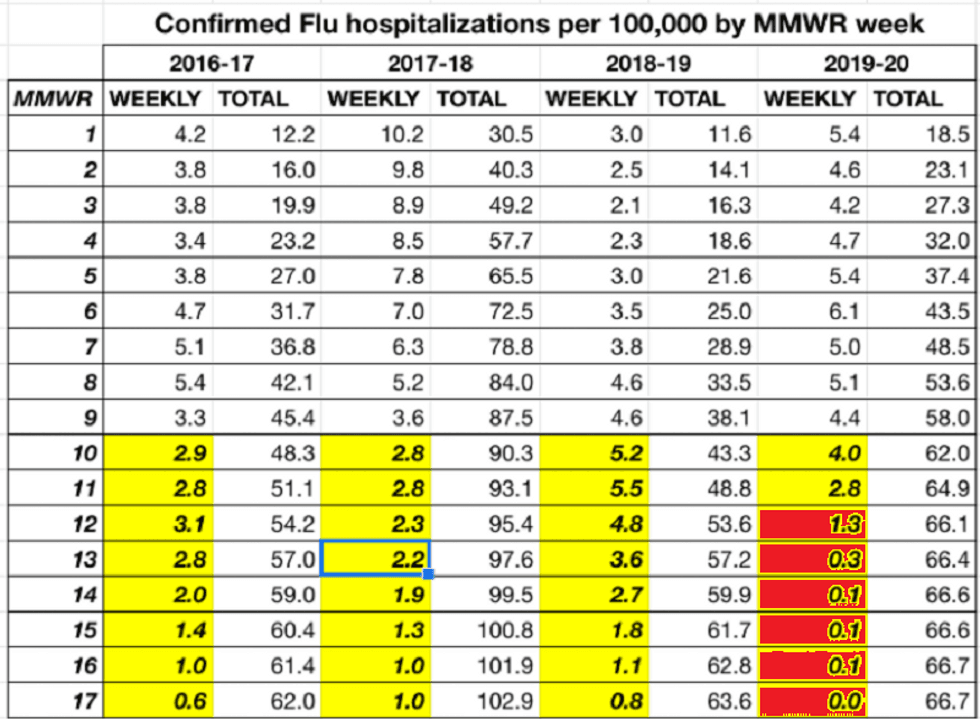 Source: Kyle Lamb
Source: Kyle Lamb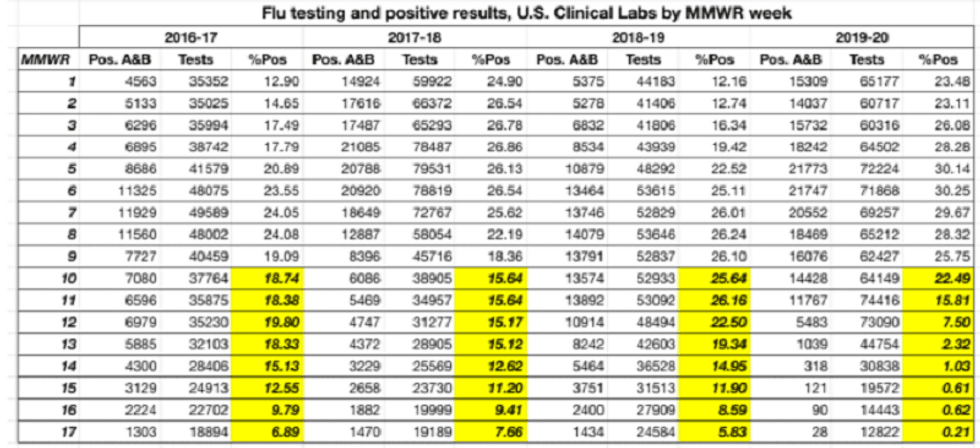 Source: Kyle Lamb
Source: Kyle Lamb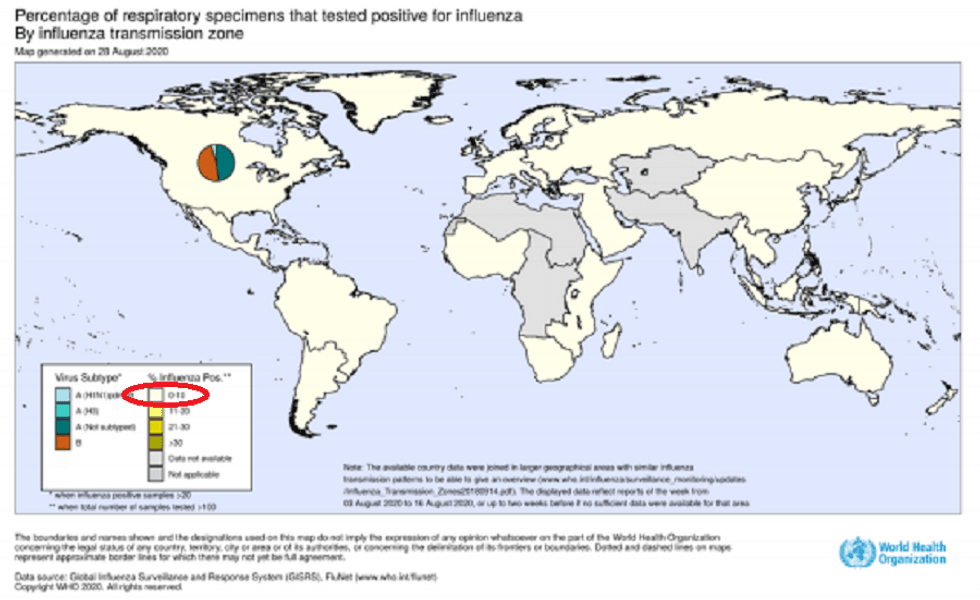 Source: World Health Organization
Source: World Health Organization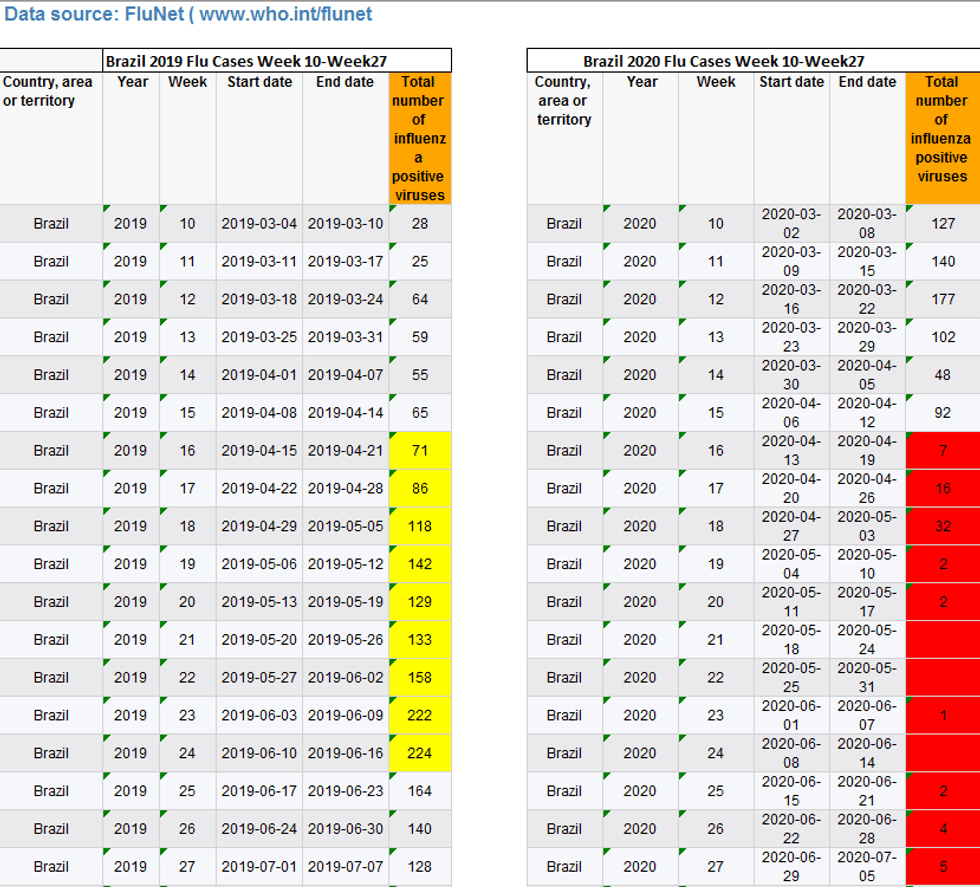 Source: Kyle Lamb
Source: Kyle Lamb