RFK Jr. shuts down $1 BILLION in funding to California and Minnesota

Health and Human Services Sec. Robert F. Kennedy Jr. said that concerns over fraud schemes have led him to shut off $1 billion of federal Medicaid spending for California and Minnesota.
Kennedy made the announcement Tuesday after noting the many schemes that had been identified and prosecuted in the two states, both run by Democrats.
'States that receive federal Medicaid funding must demonstrate that every dollar meets federal requirements.'
"Medicaid exists to serve vulnerable Americans — not to bankroll unsupported claims," Kennedy said in a press release. "Under President Trump's leadership, we are restoring accountability across our public programs and protecting taxpayer dollars."
Kennedy appeared at a media briefing alongside Centers for Medicare and Medicaid Services Administrator Dr. Mehmet Oz to explain why they halted $867.5 million in spending for California and another $199 million for Minnesota.
"States that receive federal Medicaid funding must demonstrate that every dollar meets federal requirements. When they cannot, we will not release federal funds until they do," Kennedy added.
HHS is awaiting documentation from both states to justify high-risk Medicaid claims. An analysis from CBS News found that 700 of the approximately 1,800 hospices in Los Angeles County triggered red flags for fraud, using California's definitions.
Democratic California Gov. Gavin Newsom issued a defiant statement about the decision.
"Today's announcement from Dr. Oz is the same recycled political stunt we've seen before. California isn't being targeted because Trump has evidence of fraud," he wrote on social media.
'We are being targeted for political reasons — and because Dr. Oz doesn't understand that we are *SAVING* taxpayers money by keeping seniors and people with disabilities out of far more expensive nursing homes! We hate fraud. That's not what this is. And we stand ready to collaborate with CMS in good faith efforts to combat fraud."
RELATED: Former Miss North Dakota pleads guilty to day care fraud in Minnesota
Minnesota Gov. Tim Walz (D) also responded in a brief statement to the New York Post accusing the administration of "cutting more money in health care than they've prosecuted for fraud.”
HHS said the rate of growth in claims from California's in-home care programs far outgrew the national average, suggesting some fraud was involved.
The funding paused in Minnesota involved Medicaid claims from "14 high-risk service areas."
"The Trump administration is committed to rooting out fraud, waste, and abuse across the federal government," HHS said in its statement. "HHS will continue to aggressively protect taxpayer dollars and hold states accountable for every federal Medicaid dollar they spend."
Like Blaze News? Bypass the censors, sign up for our newsletters, and get stories like this direct to your inbox. Sign up here!

 Feodora Chiosea/iStock/Getty Images
Feodora Chiosea/iStock/Getty Images At a time when multiple budget analysts have highlighted an explosion in Medicare spending due to the IRA, what did Wyden’s white paper propose? More of the same.
At a time when multiple budget analysts have highlighted an explosion in Medicare spending due to the IRA, what did Wyden’s white paper propose? More of the same.
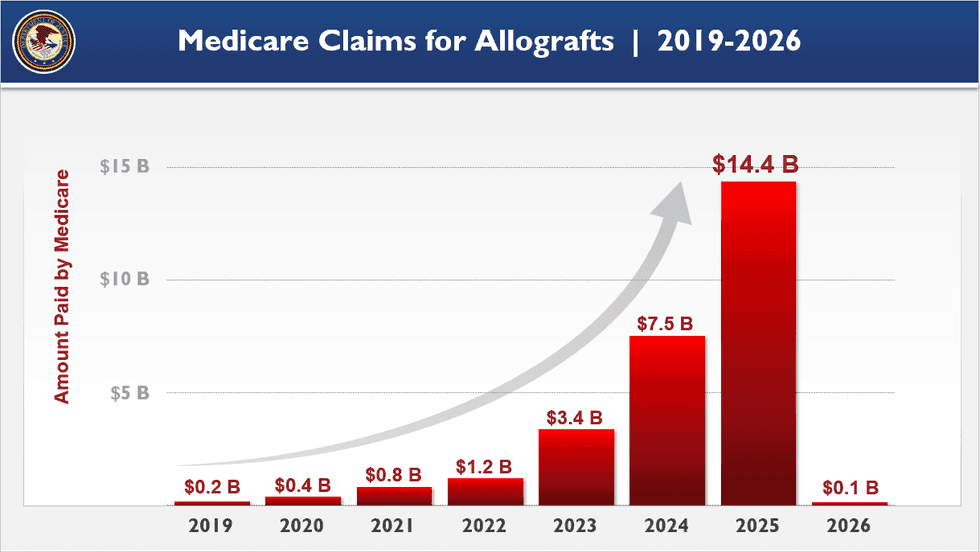 Image source: Department of Justice
Image source: Department of Justice Bulgari necklace and beach resort in the Philippines. Image source: Department of Justice
Bulgari necklace and beach resort in the Philippines. Image source: Department of Justice In avoiding political discomfort for decades, Congress and presidents have set the nation up for an economic and social catastrophe.
In avoiding political discomfort for decades, Congress and presidents have set the nation up for an economic and social catastrophe.
 Kevin Dietsch/Getty Images
Kevin Dietsch/Getty Images The Social Security and Medicare trust funds incurred a net of over $132 billion in losses in 2025 — losses that will only grow in future years.
The Social Security and Medicare trust funds incurred a net of over $132 billion in losses in 2025 — losses that will only grow in future years.
 Jim Lo Scalzo/EPA/Bloomberg/Getty Images
Jim Lo Scalzo/EPA/Bloomberg/Getty Images