Blaze News investigates: Long before COVID, Merck allegedly lied about mumps vaccine in MMR II

Litigation against pharmaceutical giant Merck regarding one of its common childhood vaccines has lingered in the court system for more than a decade even though there has been seemingly little dispute about the veracity of the fraud claims against it.
Blaze News reviewed court documents related to the Merck cases and spoke with one attorney as well as several individuals who have put together a feature film, "Protocol 7," about the allegations made in them. According to this evidence, it appears that Merck knew about problems with the mumps component of its measles, mumps, and rubella vaccine, often referred to as MMR II, in the 1990s and has spent significant resources in the decades since to cover up those problems rather than admit the truth or improve the vaccine's quality.
Merck's attorneys did not respond to Blaze News' request for comment.
A 'voice to children who have none': Context of 'Protocol 7'
The allegations dramatized in "Protocol 7" were first made by Merck employee whistleblowers in 2001 and in a federal complaint under the False Claims Act filed under seal in 2010 and made public in 2013. In 2024, questioning the government pitch about vaccines is no longer taboo, thanks in large part to the controversial COVID-19 vaccines. But skepticism about vaccines was not always so socially acceptable.
Just ask Dr. Andrew Wakefield, a British former physician and the writer, director, and executive producer of "Protocol 7." Wakefield was stripped of his medical license and shunned by many in the medical community as a "disgraced anti-vaxxer" after he suggested in the 1990s that children take separate vaccines for measles, mumps, and rubella, perhaps a year apart, because of a possible link between MMR and autism.
Wakefield told Blaze News that he doesn't much mind the attempts to ostracize him. "My production team and I have both moral and professional obligations to give voice to children who have none," he said. "Contrived and dishonest allegations against me only serve to strengthen my resolve."
Wakefield now lives in Austin, Texas, and recently appeared on BlazeTV's "Sara Gonzales Unfiltered" to talk about his experiences promoting vaccine safety and informed consent. A portion of that interview can be viewed below. Subscribe to BlazeTV for other such original content.
'Like a cold': Children and the mumps virus
Between measles, mumps, and rubella, a mumps vaccine would likely be the hardest to sell to parents if there were no MMR II on the CDC's childhood immunization schedule. For one thing, a mumps infection is rare and poses only a low risk to children. Children who do contract the disease likely experience swollen glands, muscle pain, and a fever for a week or less.
Even the CDC website admits: "Some people who get mumps have very mild symptoms (like a cold), or no symptoms at all and may not know they have the disease."
Of course, low risk does not mean risk-free, and one of the most significant risks mumps presents to children is deafness. According to Dr. Robert Malone, who became a household name in recent years because of his public criticism of the COVID vaccines but who also lent his expertise to the whistleblowers in the Merck case, "Mumps has historically been one of the leading causes of childhood deafness." Dr. Wakefield told Blaze News that, though deafness is a frightening possibility with childhood mumps, such incidents are "rare."
Once children go through puberty, however, a mumps infection becomes considerably more dangerous. Males may develop an inflammation of their testes, increasing their chances of sterility. Women who contract mumps while pregnant have "a spontaneous abortion rate of up to 25%," Malone said. In rare cases, adults who contract mumps may even develop meningitis or encephalitis, otherwise known as inflammation of the brain.
'96%' effective: Merck's MMR II vaccine
The dramatic increase in risk that mumps poses once children have aged into and beyond puberty is precisely why Wakefield calls Merck's alleged fraud regarding its MMR II vaccine so "insidious." Before 1968, nearly every child experienced a case of mumps, he said, most of which were mild and "easily treated with antibiotics." Such infections also caused children to naturally develop mumps antibodies that fortified them against re-infection in the future.
In theory, a mumps vaccine would accomplish the same end, but Wakefield, the Merck whistleblowers, and others believe that MMR II has not lived up to its billing regarding mumps. In fact, Wakefield told Blaze News that MMR II has largely been "impotent" and "ineffective" at creating sufficient mumps antibodies in children, thus leaving them at risk of a more severe mumps infection as adults.
Nevertheless, Merck first received a license for a composite measles, mumps, and rubella vaccine in 1978 and began manufacturing it en masse to sell those vaccines to the CDC, which then added MMR to its list of recommended childhood immunizations. Merck and the CDC both recommend that the first dose be administered when a child is between 12 and 15 months, and a second dose should be given when the child is between 4 and 6 years old.
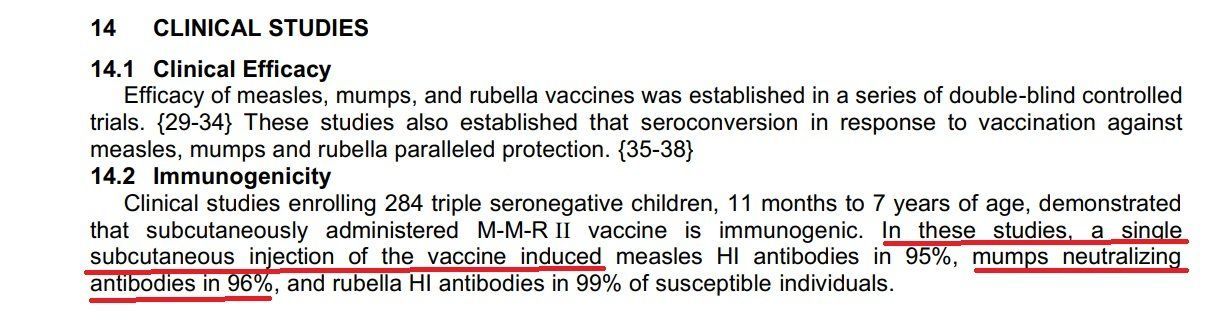
According to Merck's MMR II product insert, updated within the last year, "96%" of the children who were injected with MMR II in its "clinical studies" exhibited "neutralizing antibodies" for the mumps virus. In other words, the vaccine is 96% effective at guarding recipients against mumps infection, the company asserts.
'Out of compliance': Signs of trouble
By the mid-1990s, though, Merck allegedly learned that the MMR II vaccine could not maintain minimum potency throughout its advertised two-year shelf life. According to whistleblowers' allegations in court documents filed last November, Merck employees admitted at some point that MMR II was "misbranded," "out of compliance," and needed "immediate corrective action" to avoid a product recall.
What followed was a clinical trial that allegedly involved unethical and illegal interventions to doctor the testing and data in a failed attempt to maintain the 96% efficacy threshold. This clinical trial became internally known as Protocol 007.
The fraud allegedly perpetrated by Merck employees during Protocol 007 was brought to light by Stephen Krahling and Joan Wlochowski, former Merck virologists who came forward as whistleblowers.
Constitutional lawyer and adviser to the "Protocol 7" film Jim Moody noted that Krahling and Wlochowski are more than just whistleblowers. In court documents, they are referred to as relators, and Moody told Blaze News that as insiders who closely observed the fraud, their testimony carries significant weight in court.
"A paradigmatic relator is a close or a firsthand observer of the fraud," Moody told Blaze News. "... The courts like these firsthand relators [because these] people were in on it, if you will, saw it."
Such direct witness testimony "resolves issues about credibility" regarding the accusations because they are based on eyewitness testimony rather than, say, a "statistical analysis" of big data in state or national records, Moody explained.
'The callousness [of] this fraud': Protocol 007
According to the allegations made by Krahling and corroborated by Wlochowski, Protocol 007 quickly devolved into a series of attempts to cook the data to justify the assertion that MMR II was at least 95% effective at creating mumps antibodies in children. Wakefield told Blaze News that independent testing puts the number somewhere between 60% and 70%, and such reduced effectiveness would almost certainly end the CDC's continued purchase of MMR II, which amounts to about $100 million per year.
To avoid such financial and reputational catastrophe, the first step some Merck scientists allegedly took was to increase the sensitivity of the plaque reduction neutralization tests, which are commonly used to determine vaccine efficacy. They reportedly achieved this increased PRNT sensitivity by testing MMR II against a weakened, lab-generated strain of the mumps virus, even though a naturally occurring and more potent strain was required by law. Even with the more sensitive PRNTs, however, the Merck team apparently could not verify that the MMR II vaccine was 95% effective even against the weakened mumps strain.
The next move Merck researchers allegedly made was to inject rabbits with human antibodies and then take blood from these rabbits to create a glue that would then be added to the PRNTs, a kind of blood and antibody laundering, if you will.
The glue apparently worked — in fact, it worked too well because it created an additional problem: pre-positives on the test plates. In this case, pre-positives are samples of blood taken from children who have never been exposed to the mumps disease or received a dose of the vaccine and thus should have no mumps antibodies but who appeared to exhibit such antibodies nonetheless. As these pre-positive blood samples have already demonstrated antibodies before receiving a vaccine injection, they cannot help but verify vaccine efficacy.
At this point in Protocol 007, either out of frustration or desperation, some Merck employees allegedly decided to stop monkeying with the tests and instead change the numbers recorded in the data to reflect the desired result.
A Merck supervisor cited in court documents reportedly testified: "My goal and my understanding ... was to have [a test] that would allow us to have the capability of measuring 95 percent seroconversion ... without considering the impact on accuracy."
This alleged fraud was not just minor tweaking, court documents showed. Nor was it the result of carelessness or haste.
"Relator Joan Wlochowski testified that she witnessed counting sheets being discarded by lab staff" in connection with Protocol 007, and one Merck lab executive admitted under oath that he discarded many of the Protocol 007 testing plates before "anyone from quality assurance" could verify that they had been properly recorded, Dr. Malone noted in his report.
Indeed, a transcript from a 2017 deposition shows that the lab executive testified: "As best I recall, my understanding of this was that retention of the plates was not a requirement. That the plaque counting sheet was the primary source of the data and the [testing] plates were not -- wasn't required to retain them as the primary data source."
Dr. Wakefield told Blaze News that to add interest and intrigue to the movie "Protocol 7," he and the other writers actually added a "moral quandary" for the character representing this Merck lab executive that he might not have experienced in real life. Otherwise, Wakefield said they risked audiences becoming suspicious that the malfeasance of the Merck figures had been exaggerated.
Moody, legal adviser to the film, indicated to Blaze News that Merck's culpability cannot be overstated.
"The case itself revealed multiple instances, repeated instances of over and over and over again of other frauds," he insisted. "... It's just the callousness by which this fraud was done that makes [Merck], in my view, the extent of the villain that they are."
'Raw data is being changed': The FDA inspects Merck lab
As the licenser of vaccines, the FDA has a keen interest in vaccine data and efficacy as well.
In August 2001, Krahling, one of two relators in the cases against Merck, contacted the FDA to report the fraud he had allegedly witnessed, even though his superior had reportedly threatened him with termination, and he was also allegedly threatened with possible jail time if he came forward. The FDA then alerted Merck about possible deficiencies in the data collected in the Merck executive's lab, court documents said.
The FDA also made an "unannounced" visit to the lab within days of Krahling's report, though Wakefield and his fellow filmmakers indicated that an FDA source may have tipped Merck off about the visit. In any case, the result of the visit was damning for the company.
"Raw data is being changed with no justification," said an FDA Form 483 signed by Debra Bennett and Dr. Kathryn Carbone, according to court documents. An FDA Form 483 is issued "when an investigator(s) has observed any conditions that in their judgment may constitute violations of the Food Drug and Cosmetic Act and related Acts," the agency's website states.
In addition to problems with the raw data, that FDA form also noted potential problems with the Merck executive's lab, the "spreadsheets used to determine questionable results and retesting of clinical samples," and the "notebooks" that logged the individuals "performing each task."
'Materiality': Merck litigation focused on money
Despite the alarming report from the FDA, Merck continued to manufacture MMR II and sell it to the CDC. So in 2010, nearly a decade after the FDA inspection at the Merck lab, relators Krahling and Wlochowski sued Merck under the False Claims Act, which relates to occasions in which the government may have been monetarily defrauded, Moody — a false claims lawyer — told Blaze News.
The case has languished in the court system for the past 14 years, but both sides eventually tried to propel it toward a resolution by filing a summary judgment, which allows one or both sides to argue to a judge that they are entitled to win without submitting the case to a jury because there is allegedly no dispute on the facts or law.
A summary judgment hearing was then held in the Merck case in January 2023, but Merck's legal team did not really seize the opportunity to defend the company against the allegations of fraud. Instead, the "most obvious and undisputable ... reason to grant summary judgment for Merck," Merck attorney Jessica Ellsworth argued at the hearing, was "materiality," a transcript showed. Ellsworth explained materiality in this case to be whether the "CDC would have made different purchasing choices in the Vaccine for Children Program" had it known about the alleged problems with MMR II.
Ellsworth claimed plaintiffs offered "no non-speculative evidence that CDC would have made any different purchasing choices related to M-M-R II based on Relators’ opinions about a research study known as Protocol 007." She also called any suggestion to the contrary "speculation" and "innuendo."
District Judge Chad Kenney of the Eastern District of Pennsylvania agreed, ruling last July that "considering the totality of the circumstances, no reasonable jury could conclude that the alleged false claims were material to the CDC’s purchasing decisions."
That failed False Claims Act case as well as a separate antitrust class action against Merck are now both in the hands of the Third Circuit Court of Appeals and will be decided jointly. Oral arguments in the appeals cases could be held as early as next month.
Lead attorneys for relators Krahling and Wlochowski did not respond to Blaze News' request for comment.
'Vigorously dispute': Merck issues a formal response
While Merck's attorneys focused on materiality as the basis of their defense of Merck in court and have never actually responded to the allegations of fraud publicly, Merck has issued a defense of sorts for MMR II and its research and development. That defense came in response to allegations from former FDA Commissioner Dr. David Kessler, who served as an expert witness for relators Krahling and Wlochowski.
In addition to restating concerns regarding Protocol 007, in a letter dated August 2019, Kessler expressed concerns about incidents of "low mumps potency" MMR vaccinations. In the four short years between 1995 and 1999, Merck reportedly estimated that it had issued 23 million such "low mumps potency" MMRs. After analyzing the same data based on "Merck's methodology for identifying the 23 million doses," Kessler claimed he found that the number was actually closer to 60 million.
Kessler, who described himself as "a strong proponent of vaccines," worried that 60 million "doses of potentially sub-potent vaccine" might "shake the public's confidence in vaccines generally and measles, mumps and rubella vaccine specifically." Nonetheless, Kessler recommended that Merck and/or the government inform patients that they had received an ineffective mumps vaccine, undertake further studies and medical monitoring, and consider developing a new mumps vaccine.
In return, Merck issued a letter that boasted about MMR's overall success at reducing measles, mumps, and rubella infections. The letter also indicated that many of the alleged potency problems associated with the vaccines manufactured before September 1999 could be attributed to a change in "interpreting the potency label claim." "This change was not related to product performance, nor did it present a clinical issue or otherwise create a basis for clinical concern," Merck asserted.

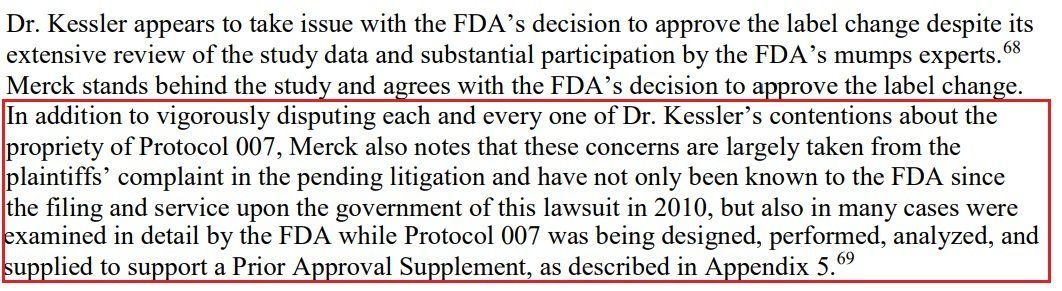
Elsewhere in its response letter, Merck did mention Protocol 007, claiming to "vigorously dispute[] each and every one of Dr. Kessler’s contentions about the propriety of Protocol 007" and insisting that such contentions were based on "plaintiffs’ complaint in the pending litigation." Not only has the FDA known about "concerns" regarding Protocol 007 since at least 2010, Merck's letter claimed, but the FDA had actually "examined" those concerns "in detail ... while Protocol 007 was being designed, performed, analyzed, and supplied to support a Prior Approval Supplement."
Wakefield told Blaze News that such assertions still do not explain "the multiple outbreaks of mumps in highly vaccinated populations." Merck's attorneys did not respond to Blaze News' request for comment.
'As many as 94 percent of those who contracted the illness had been vaccinated"
While cases against Merck have lumbered about in the court system, mumps outbreaks have made a minor resurgence in America. In 2016 and 2017, a period that a 2021 NBC News article called the "peak" of this resurgence, 37 states and Washington, D.C., experienced small pockets of outbreaks that resulted in 9,000 reported mumps cases, a tremendous jump from the 231 cases reported in 2003.
NBC News further noted that two-thirds of all reported mumps cases between 2007 and 2019 occurred in people who had aged beyond adolescence — meaning the disease put them at acute risk — and "as many as 94 percent of those who contracted the illness had been vaccinated."
Though no direct link has been made between possible issues with the MMR II vaccine and the increases in mumps cases, Dr. Wakefield and the rest of the "Protocol 7" team believe that because Merck allegedly altered so much key data decades ago, without testing, it's nearly impossible now to determine whether adults who received MMR II as children since the time of Protocol 007 continue to have immunization against mumps — if they ever had immunization in the first place.
According to Wakefield, those children who received an ineffective dose of MMR II would be "in danger of catching mumps as a teenager and older, when mumps is a much more serious disease."
The CDC recommends that "adults who do not have presumptive evidence of immunity should get at least one dose of MMR vaccine." Some may require two doses, the agency says.
While the CDC continues to recommend and purchase MMR II from Merck, the agency has quietly put a competing MMR from GlaxoSmithKline on the schedule and is starting to switch purchases, the "Protocol 7" team told Blaze News.
'Doubts ... cannot be allowed to exist': Big Pharma set up for success
Like all major pharmaceutical companies, Merck seemingly enjoys the benefit of the doubt from the U.S. government. Since at least the early 1980s, the federal government has been openly worrying about public trust in vaccines manufactured by Merck and others, claiming that such vaccines are the safest way to achieve herd immunity for many dangerous diseases.
A June 1984 federal register discussing the polio vaccine went so far as to say that "any possible doubts, whether or not well founded, about the safety of the vaccine cannot be allowed to exist in view of the need to assure that the vaccine will continue to be used to the maximum extent consistent with the nation's public health objectives."
The polio immunization program "depends on" "maintaining public confidence," the register continued, so the FDA ought not to revoke the polio vaccine license based on "deficiencies in the lots" used to test the polio vaccine's efficacy.
Within a few years of that federal register about the polio immunization program, pharmaceutical manufacturers like Merck gained the added benefit of immunity against vaccine injury tort liability in most individual cases, thanks once again to the federal government. U.S. Code provides that "no vaccine manufacturer shall be liable in a civil action for damages arising from a vaccine-related injury or death associated with the administration of a vaccine after October 1, 1988, if the injury or death resulted from side effects that were unavoidable even though the vaccine was properly prepared and was accompanied by proper directions and warnings."
Critics of the COVID vaccines released at the tail end of the Trump administration pointed to even broader protections granted to the industry under the 2005 Public Readiness and Emergency Preparedness Act and the COVID emergency declarations, noting that because of such far-reaching immunity, Pfizer, Moderna, and Johnson & Johnson likely would never be held financially responsible for injuries and death caused by the COVID vaccines. The only exception the PREP Act offers against this blanket immunity is "willful misconduct."
'That's winning': Finally, open dialogue about vaccines
The sharp divide regarding the efficacy of the COVID shots stands in stark contrast to the general acceptance of MMR in most parts of the Western world. But even though billions of doses of COVID shots have been administered worldwide in the past few years, Dr. Wakefield still sees the controversy over COVID vaccines as, in some respects, a victory for vaccine safety and open debate more broadly.
"The majority of adults, certainly in [America], will not get any booster," he told Blaze News. "They said, 'We're done. We're not doing any more.' ... So we now have gone from a handful of people ... who've tried to talk about [vaccine safety] to a majority of the adult population, certainly in this country and essentially the world.
"And that's winning."
However, Moody noted somberly that the change in discourse came in large part because of "constantly shifting and evasive government positions, outright lies, and a near-complete lack of transparency and cover-up of injury and death data."
Still, millions of American children have received the MMR II vaccine without experiencing any adverse side effects or ever developing mumps. Wakefield, Moody, and the others who spoke with Blaze News reiterated that they are not against all vaccines. They simply want consumers, especially parents, to have all the information they need to make the best decisions for themselves and their families and to be able to make these decisions without pressure or coercion from the government, the manufacturers, or the public. They also call for a repeal of blanket immunity for vaccine manufacturers and swift and generous no-fault compensation for all the victims of what they call "the war against disease."
In Wakefield's words, "It's all about informed choice."
Like Blaze News? Bypass the censors, sign up for our newsletters, and get stories like this direct to your inbox. Sign up here!