What happened to RFK Jr.’s red line on risky vaccines?

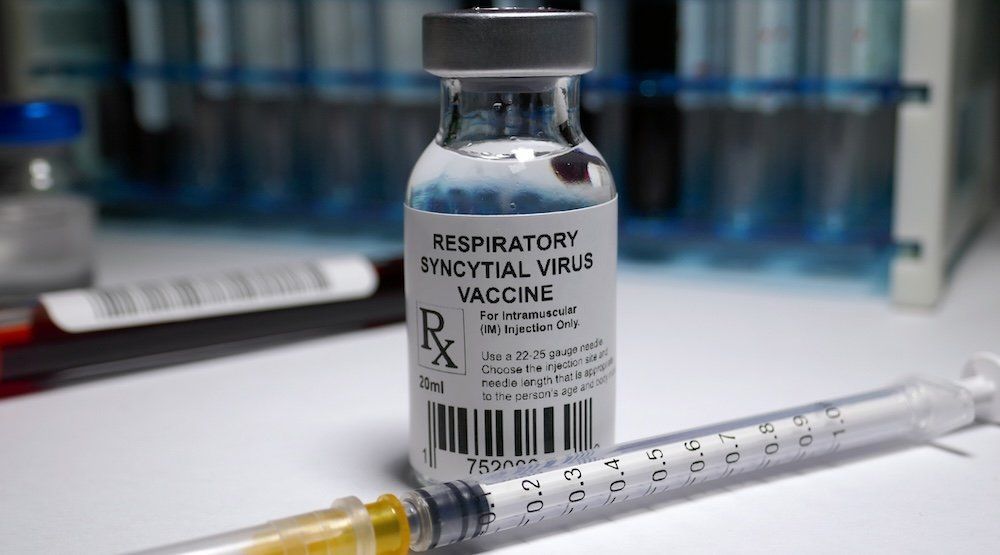
For nearly half a century after the catastrophic 1967 trial, the U.S. government failed to approve a safe and effective RSV vaccine. Then came the COVID-19 debacle — and suddenly, we’re supposed to believe the science caught up. As if by magic, after the mRNA disaster and its lingering questions, federal agencies now bless an endless stream of RSV shots for children and adults alike.
Never mind that just two years ago, Anthony Fauci co-authored a paper admitting that safe RSV vaccine development faced “many and complex” challenges. He cited risks like antigenic drift and called for “outside-the-box” thinking to make next-generation vaccines possible.
If Kennedy truly doubts the safety of older vaccines, why would his handpicked advisers endorse new injections for a virus that rarely warrants immunization?
Apparently, that box got checked quickly — at least according to the Centers for Disease Control and Prevention.
The CDC’s Advisory Committee on Immunization Practices voted last month to approve Merck’s new RSV monoclonal antibody shot, Enflonsia, for prophylactic use in infants. The treatment mimics a vaccine in function and application.
The approval came despite glaring trial results.
Yes, the Phase 2b/3 CLEVER trial included a legitimate placebo group — finally. But the vaccinated group suffered more deaths and injuries than the placebo group. All-cause mortality ran slightly higher among those who received Enflonsia.
How can any vaccine win approval without reducing the risk of death?
Trial data showed three deaths linked to the vaccinated group, compared to just one among the placebo group. Statistically underpowered or not, that outcome suggests a 50% higher risk of death. That alone should have triggered demands for further study.
Instead, the CDC approved it.
The vaccinated group also faced a 350% higher incidence of upper respiratory tract infections, a 63% higher rate of lower respiratory infections, and a 41% higher risk of febrile seizures. The sample size wasn’t large enough to detect rarer events — yet regulators waved it through anyway. And all this for a virus that most infants overcome with basic care and a nebulizer.
ACIP passed the recommendation 5-2 on June 26. Dissenters Retsef Levi and Vicky Pebsworth cited the higher death rate and adverse reactions. Levi raised additional concerns about immune enhancement — where vaccination worsens the disease in later exposure — and called for longer trials focused on high-risk groups.
History supports his skepticism. In the 1960s, trial participants who received the RSV vaccine developed worse outcomes in subsequent years. We’ve seen similar patterns with some newer RSV formulations. None of today’s trials followed participants long enough to rule out antibody-dependent enhancement.
Even Moderna’s RSV/hMPV combo trial in infants aged 5 to 8 months had to be halted last year due to signs of enhanced respiratory disease. Yet, in May 2024, the Food and Drug Administration approved a similar mRNA shot for adults 60 and older. On June 12, Trump's Health and Human Services expanded that approval to adults over 18 deemed “at risk” — despite all we’ve learned about the dangers of mRNA and respiratory virus vaccines.
RELATED: RFK Jr. torches vaccine panel to make consequences count again
The FDA under Joe Biden approved Abrysvo, Pfizer’s RSV vaccine for seniors and pregnant women, despite serious warning signs. Post-licensure data linked the shot to elevated risks of Guillain-Barré syndrome within 42 days of injection. And in trials involving pregnant women, 5.7% of infants were born prematurely in the vaccinated group — compared to 4.7% in the placebo group.
HHS Secretary Robert F. Kennedy Jr. deserves credit for demanding more rigorous placebo-controlled trials. But what’s the point if agencies approve vaccines even when trials raise red flags?
RFK Jr. has publicly questioned links between childhood vaccines and autism — especially the hepatitis B shot. If he truly doubts the safety of older vaccines, why would his handpicked advisers endorse new injections for a virus that rarely warrants immunization?
Merck’s Enflonsia includes genomic material derived from an ovarian cancer cell line. Why on earth would we inject even a minimal amount of tumorigenic cells for a bad cold that we’ve been treating successfully with a nebulizer for years?
No one expects RFK Jr. to overhaul the CDC overnight, especially given internal resistance and pro-mRNA holdouts within the White House. But at the very least, many hoped the reckless approval of unnecessary vaccines would stop under his watch.
Instead, the CDC pressed forward with the same reckless momentum.
What happened to “first, do no harm”?
 Americans know Fauci as a fraud who has done irreparable harm to our people and our nation. Will he be held accountable?
Americans know Fauci as a fraud who has done irreparable harm to our people and our nation. Will he be held accountable?

 Utah Department of Health
Utah Department of Health