You Just Have A Cold. Don’t Give Branch Covidians Their Numbers By Testing
 Don’t get tested, don’t self-report, and don’t be a statistic for the neurotic control freaks who emerged in the past few years.
Don’t get tested, don’t self-report, and don’t be a statistic for the neurotic control freaks who emerged in the past few years.A Calgary-based family physician and urgent care doctor appeared on Canadian state media earlier this week to explain the alleged link between influenza, infection, and stroke.
When explaining the linkage, Dr. Raj Bhardwaj of the University of Calgary noted his recent surprise at discovering that there is now reportedly a "stroke season."
Bhardwaj told CBC Calgary News that a stroke is ultimately when "the blood supply to the brain is compromised for some reason. It's basically a plumbing problem in the pipes that supply blood to your brain. And there's two things that could go wrong with pipes, right: they can get blocked or they can burst."
Systemic inflammation resultant of influenza can reportedly help trigger these plumbing issues.
"It can make the inside of the pipes stickier. It can make your blood a little bit thicker, especially if you get dehydrated. And it can even put the heart into a weird rhythm called atrial fibrillation," said Bhardwaj. "All of those things can increase your risk of having a stroke."
While Bhardwaj was cognizant of the potential link between flu and stroke, he was nevertheless caught off guard by the alleged existence of a "stroke season."
"I didn't know about this either until last year, but it turns out that after flu season, about three or four weeks later, there is a stroke season," he said. "Most of Canada is getting down off of a big hump of flu, so now we're starting to see more strokes."
Bhardwaj noted that he was not the only doctor in the dark about so-called "stroke season."
"One of my colleagues actually mentioned that at work the other day and said, 'Have you noticed how many strokes we're seeing? It's a lot more than usual it feels like,'" said Bhardwaj. "Anecdotally, we're starting to see that."
\u201cHoly shiat\u2026 \u201cI never knew there was a stroke season after flu season, until my bosses & big Pharma told me there is a stroke season after flu season\u201d. \n\nSo am I now allowed asking if people collapsing on air is a stroke? It\u2019s the season, after all, right?\u201d— Viva Frei (@Viva Frei) 1674316228
Bhardwaj claimed the "good news is that getting your flu shot reduces your risk of stroke," citing a study from the University of Calgary where he works as a clinical assistant professor.
The study in question, published in the Lancet in November, noted that influenza "is a common respiratory infection that precedes stroke."
Dr. Michael Hill, one of the authors on the study, told Global News, "There’s a longstanding history between infections and stroke — upper respiratory tract infections are associated with stroke — so it was sort of natural to start to look at this."
The study suggested that after adjusting for demographics and comorbidities, "recent influenza vaccination significantly reduced the hazard of stroke"; an association that "persisted across all stroke types."
Stroke was found to have been reduced across all ages and risk profiles with the exception to those without hypertension.
CTV News reported in December that one Canadian hospital had, like Bhardwaj's colleague, observed a "15 per cent increase in the number of stroke patients arriving ... in the first six months of this year."
"What we're seeing is that there is this measurable increase in in the risk of strokes, and not only that, but also just poor outcomes for patients that have strokes during the winter time," said physician George Dresser.
Dresser suggested that regular exercise, reduced sodium and alcohol intake, and a potassium-rich diet could help remedy hypertension and, in turn, deter stroke.
Christmastime sloth and treats may not be the only triggers of spikes in stroke, however.
A 2016 study published in the Journal of Stroke and Cerebrovascular Diseases suggested that "lower average temperature and larger diurnal temperature variations were associated with stroke hospitalizations."
Dr. Roberto Alejandro Cruz, a neurologist with DHR Health, told KRGV in May 2021 that he had noticed a spike in patients 30 years and older who had suffered strokes since the start of that year. The CDC noted that over 200 million COVID-19 vaccine doses had been administered in the United States by April 21.
While this particular study might help explain a wintertime or early spring "stroke season," researchers behind a 2019 study published in the Journal of Stroke & Cerebrovascular Diseases suggested hot temperatures might otherwise trigger strokes.
They observed "an increase in [ischemic stroke] rates relative to [intracerebral hemorrhage] during the summer months with higher solar radiations that cannot be explained by physiological measures suggestive of dehydration or hem-concentration."
Seasonal weather patterns might account for strokes, but not necessarily an significant uptick in cases.
The New York Times recently reported that data from the "Vaccine Safety Datalink, a federal safety surveillance system, hinted that Americans aged 65 and older might be at increased risk of an ischemic stroke in the 21 days after receiving" the bivalent booster shot.
The CDC — which the majority of respondents in a recent Rasmussen Report poll indicated they want investigated by Congress for its handling of vaccine safety — has announced that it is investigating whether the Bivalent Pfizer-BioNTech has increased some recipients' risk of stroke. Despite the investigation, the CDC maintains that the risk posed by the booster is "very unlikely."
Days after the CDC announced its investigation, Kate O’Brien, WHO director of Immunization, Vaccines and Biologicals, claimed that "the best evidence is that there is no true association between the booster doses of Pfizer in the older adults and strokes."
A scientific review published June 2022 in the Journal of Stroke and Cerebrovascular Diseases noted that "Most of the evidence pertaining to stroke following COVID-19 vaccination are case reports, therefore, the incidence of stroke after COVID-19 vaccination is not precisely known."
The review added that "Most patients who suffered from stroke after COVID-19 vaccination were women, under 60 years of age, and after the ChAdOx1 nCoV-19 vaccine."
Like Blaze News? Bypass the censors, sign up for our newsletters, and get stories like this direct to your inbox. Sign up here!
Those people who got a flu shot ahead of the 2019-20 flu season were reportedly less likely to suffer from severe COVID-19 requiring emergency room services, according to ABC News, citing a new report from medical journal Plos One.
New research states that people who got a flu shot may be "less likely to suffer a severe COVID-19 infection down the road."
Plos One's research, which was published Wednesday, took into consideration medical records of more than 74,700 COVID-positive people across the United States, United Kingdom, Italy, German, Israel, and Singapore.
Researchers determined that those people who had previously received the influenza vaccine during the previous six months were "less likely to have had health complications related to their COVID-19 infection."
Findings noted that those people who did not receive flu shots were up to 20% more likely to be admitted to the ICU, up to 58% more likely to visit the emergency room, up to 45% more likely to develop sepsis, up to 58% more likely to have a stroke, and 40% more likely to develop deep vein thrombosis when compared to those who had received an influenza vaccine.
The research, according to the outlet, corroborated the findings of several previous studies that found links between "better COVID-19 outcomes and flu shots."
"That prior research similarly didn't find the flu vaccine offered any protection against COVID-19 death," the outlet added. "Importantly, the flu shot's link to better COVID-19 outcomes doesn't necessarily mean it's protective against the novel coronavirus. While it's possible that the flu shot boosts immunity, it's also possible that people who opt to get the flu shot tend to be healthier overall than people who skip it, meaning they're already at lower risk for COVID-19 complications."
It remains unknown whether the flu shot — which changes annually — will have the same effect for the upcoming flu season.
In the research, study authors concluded, "Even patients who have already received SARS-CoV-2 vaccination may stand to benefit given that the SARS-CoV-2 vaccine does not convey complete immunity."
Based on the illegal, immoral, and illogical responses to the virus by state governors, we will have to suspend civil and religious liberty, destroy schooling for children, and crush the economy every flu season. For that matter, it appears that COVID-19 is indeed this year's version of the flu. And the notion that one can prevent the spread of this virus is just as illogical as an assumption that suspending democracy can arrest the spread of the flu.
Among the many important data points that are not being disseminated to the public, perhaps the most important one is the disappearance of the flu. As I noted at the end of October, the numbers are simply remarkable, and now we have more data showing the disappearance of the flu from what is normally the beginning of the new flu season.
According to the CDC's "Influenza Surveillance Report," there have been just 227 lab-confirmed flu cases in the entire country for the first five weeks of the flu season – from week 40 through week 44 (ending Oct. 31). While it's still very early in the season, at this point last year, there were already 2,851 confirmed positive cases. Phil Kerpen, president of American Commitment, tallied the five-year average through week 44 and found that the numbers are down roughly 90%.
@ImpactForward @AlexBerenson @MLevitt_NP2013 @jhaskinscabrera We're at 0.18% positive so far this flu season nation… https://t.co/AZW2rocUqP— Phil Kerpen (@Phil Kerpen)1605068354.0
The positivity rate is just 0.18%, compared to 2.68% last year. That means the positivity rate so far is down 93% from last year, even though the number of flu tests increased by 22%. So it's not like we've forgotten about testing for the flu.
The implication of this cannot be overstated. The problem with a new epidemic is that it strains the hospitals over and beyond the baseline level of visits they must contend with from other ailments. However, if the flu has essentially disappeared for this year, then COVID will be the only flu. Most of the pneumonias and other complications that result from the flu will not occur this year. Thus, when they count the number of COVID-19 patients in hospitals and use that number as pretext for panic, fear, and control, they are not giving you the total net number of extra patients in the hospitals with respiratory viruses relative to other years.
The following map from Kaiser Family Foundation is being disseminated across the internet to instill panic across the nation:
When "hotspot" ceases to become a useful concept.https://t.co/m262LZY2Ie https://t.co/ZUxhPCFqtv— Larry Levitt (@Larry Levitt)1605113732.0
What they fail to realize is that this demonstrates that COVID-19 is indeed this year's flu. It is everywhere and is instead of, but not in addition to, the flu. This is the time of year when hospitals begin to fill up. Also, the fact that this is occurring everywhere demonstrates that there is nothing you can do to stop its spread and that when the time for its seasonal spread is up, it will stop. Every state, regardless of its "mitigation strategies," is getting hit. That includes the overwhelming majority of states that have had universal compliance with mask mandates for months on end. As we can see from the map, our ability to stop this virus is no greater than our ability to stop a typical seasonal flu. So much for masks being better than vaccines.
The good news is that the overwhelming majority of those infected don't become clinically ill from the virus. Yes, there will be hot spots of places that did not initially get much saturation of the virus. Places like the Dakotas barely had any exposure for six months. The fact that they have more concentration now is merely the other side of the coin of places like New York that had a ton of cases in the spring and fewer cases now. Yet even in those places, how many are truly in the hospital because they have trouble breathing from a severe case of this virus?
North Dakota now has the highest case level per capita. So, are the hospitals really overrun? Unlike other states, the N.D. government breaks down the number of people who are hospitalized because of COVID vs. those in the hospital because of other ailments with COVID (simply because they tested positive while already in the hospital). If you look at those who are actually hospitalized because of COVID-19, they account for 15% of the hospital beds.
Every area that never got hit will suffer about 6-8 weeks of higher hospitalizations. But everywhere else, it will be on par with the flu season, given the disappearance of the normal flu. Let's not forget that as 67,000 people are currently hospitalized with COVID (not all because of it), there were an estimated 810,000 hospitalized with the flu during the 2017-2018 season. That means the peak of that season in January 2018 was likely much worse than today. And hospitals didn't get $200 billion from the federal government to deal with it like they do today. Nor did they test for the flu as much as they test for COVID.
"The 2017-2018 influenza epidemic is sending people to hospitals and urgent-care centers in every state, and medical centers are responding with extraordinary measures: asking staff to work overtime, setting up triage tents, restricting friends and family visits and canceling elective surgeries, to name a few."
Those were the opening lines of a Time Magazine article published January 18, 2018. Not ancient history. Yes, it was a stressful time for health care workers, but the country at large was unaware of it and there were no disruptions to life ordered by government, much less suspension of civil liberties. That is all going to change henceforth … if we allow this to continue."Twindemic."
It's the new literary expression of panic being propagated by politicians and public health officials as pretext for continuing the social control measures indefinitely. If you search for the term "twindemic," you will find all sorts of ominous predictions of a "perfect storm" of a raging coronavirus pandemic converging with a harsh flu season to overrun the hospitals and pile up the bodies in the morgues. There's just one problem: We've already had COVID-19 for at least nine months, and we've seen that this virus and the seasonal flu do not proliferate together.
My friend Kyle Lamb, the ultimate COVID-19 math and data guru, has been messaging me for months about the strange phenomenon of the disappearance of the flu in the Southern Hemisphere. The issue didn't grab my interest at first because the public health elites hadn't begun to sow panic about the coming flu season in our hemisphere yet. Then, on Sept. 18, the CDC published a paper acknowledging that the flu had essentially disappeared from the Southern Hemisphere this past summer. That is an astoundingly positive fact that almost everyone in the world is unaware of amid the endless barrage of doom and gloom in the news.
The World Health Organization has observed that overall "influenza activity remained record low in comparison with previous seasons." The WHO discovered an almost miraculous cure for the flu! "Despite continued or even increased testing for influenza in some countries in the southern hemisphere, very few influenza detections were reported," wrote the WHO in an Aug. 31 report on influenza surveillance data.
The numbers are truly remarkable. In Australia, for example, there were just 107 lab-confirmed cases of influenza this past August, as opposed to 61,000 in August 2019. The same dynamic was observed in countries like South Africa, Chile, and Argentina – all countries that get their flu season during the North American summer.
@kerpen Data from Chile. Flu and other resp viruses disappeared last southern winter https://t.co/I4xQJ8YLb0— Robinson Nuñez (@Robinson Nuñez)1602732250.0
A recent study by Australian researchers found "98.0% and 99.4% reductions in RSV [respiratory syncytial virus] and influenza detections respectively in Western Australian children through winter 2020; despite reopening of schools."
Those numbers are simply astounding and hint to some strong immunobiological phenomenon more than any human intervention as the culprit. It seems clear that when there is a dominant respiratory virus in circulation, it predominates over the flu and possibly other respiratory viruses. To test this theory, I asked Kyle to dig into data from the U.S. in the late winter. I recalled numerous articles early on in this past flu season warning of a moderate to severe season, but then it seemed to die off in February, and we wound up with just 22,000 reported flu deaths, the lowest in a decade. Could it be that we had already experienced the disappearance of the flu once COVID-19 began circulating more widely in early March?
The answer is a resounding yes!
After compiling the CDC's data on weekly influenza hospitalizations per 100,000 for the three prior flu seasons, Kyle contrasted those numbers to the weekly trend line in the 2019-2020 season. The numbers are astonishing:
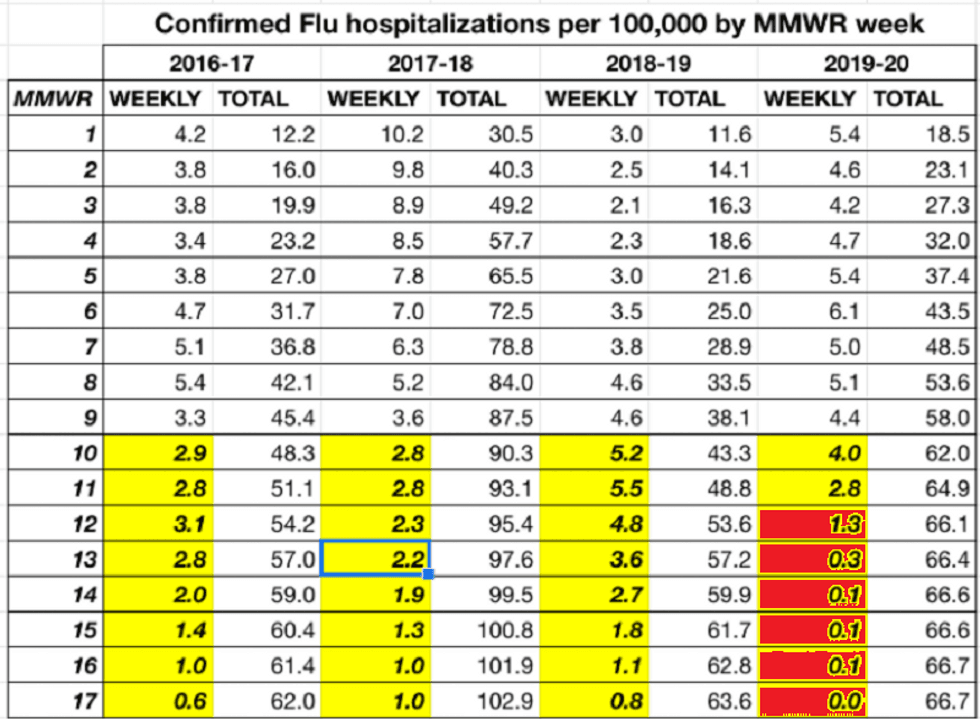
As you can see, every year, the flu season begins to wane around week 10 (ending March 7, this past year) until it is essentially over around week 17 – at the end of April. But if you look at the 2019-2020 flu hospitalization data, you will notice that the flu didn't just wane in March, it died precipitously. By week 13 (ending in early April), the hospitalization rate was much lower than during any year on week 17, when it's normally the lowest and people are thinking a lot more of spring allergies than the flu!
Thus, we have already experienced this phenomenon of coronavirus cancelling out the flu in the Northern Hemisphere, but few have noticed it.
You might suggest that the lower numbers of confirmed hospitalizations were only evident because we were so focused on coronavirus at that point and weren't testing for the flu, even though it might still have been circulating, but not captured in the data. Kyle has the data on that as well:
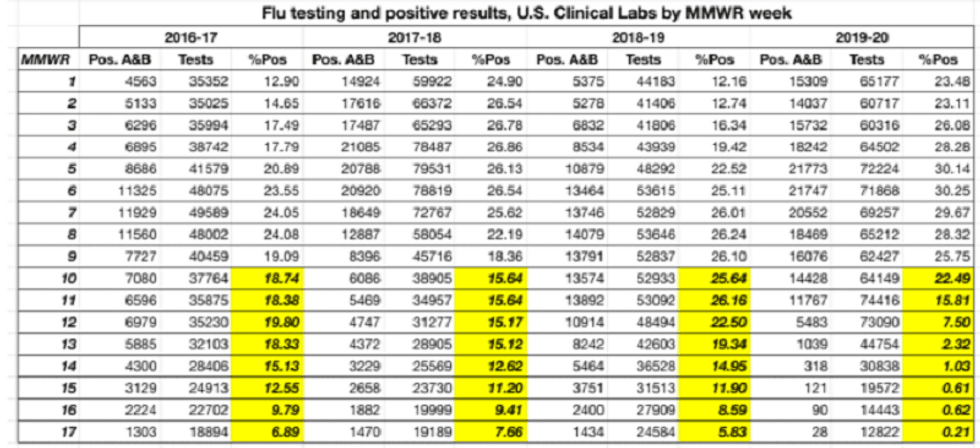
As you can see, we actually increased flu testing well over the numbers of any previous year. This was likely due to the fact that in February and March, there were limited numbers of COVID-19 tests available and hospitals were actually liberally testing for the flu as a means of ruling out other pathogens and better diagnosing COVID-19. Yet despite the increased tests, the rate of positivity for the flu plummeted to near zero. In April, the positivity rate for flu tests hovered between 1/20 and 1/40 of the rate from the past three years!
Let's come full-circle back to the present. We stand today at the precipice of the new flu season – 2020-2021. Based on CDC data for week 40 of this year, we are already seeing the miraculous decline in the flu:
Flu Testing, 2020 Week 40 vs. 2019 Week 40Clinical labs:2020: 17 positives on 7,923 tests (0.21%)2019: 447 posi… https://t.co/A6nD0aMJo8— Phil Kerpen (@Phil Kerpen)1602729931.0
Thus, it is now an undeniable fact that COVID-19 essentially has not only reduced the prevalence of influenza, but it has nearly boxed it out of existence in both hemispheres. The big question is why. The CDC and WHO reports on the disappearance of the flu are extolling the virtues of "mitigation efforts," such as mask-wearing, social distancing, and better hygiene as the key to defeating the flu.
The CDC believes the decline in the flu is due to "widespread adoption of community mitigation measures to reduce transmission of SARS-CoV-2." Likewise, the WHO suggests, "The various hygiene and physical distancing measures implemented by Member States to reduce SARS-CoV-2 virus transmission have likely played a role in reducing influenza virus transmission."
Let's just indulge this point for a moment as if it were true. That would be an admission that these efforts have failed to block COVID-19 but somehow stopped the flu from circulating. It's a truly bizarre assertion.
Fortunately, you don't have to engage in mental gyrations to figure out why these measures would work for one respiratory virus and not the other, because several simple facts demonstrate that natural predominance of COVID-19, not human intervention, is what stopped the flu from circulating widely during the pandemic.
The reality is that lockdowns didn't begin until the end of March, and the universal mask-wearing was implemented several weeks to several months later, depending on the region. Plus, it takes a few weeks for these measures to register, assuming they work. Only the natural immunobiological phenomenon of one circulating virus pushing aside another would explain why the flu died in early March.
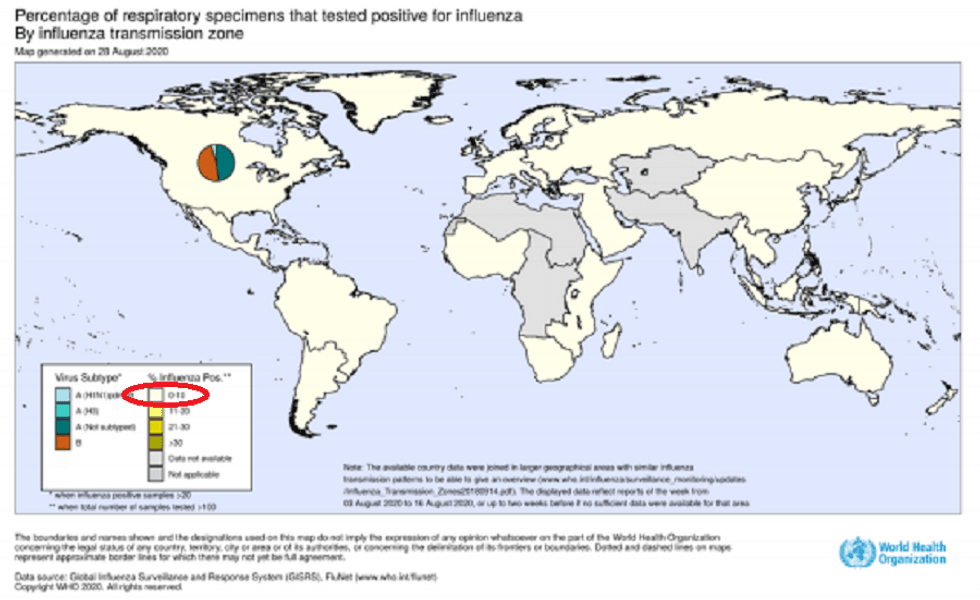
Moreover, the flu disappeared from nearly every country, not just the ones that exercised these attempted mitigation efforts. In typical years, the positivity rate of flu testing reaches well over 10% in most countries, yet the WHO reported that not a single country had more than a 2%-3% positivity rate this year.
Ironically, one of the only countries that did have a flu outbreak at the tail end of the summer this year was Cambodia, but as Kyle points out, the country barely had COVID-19 cases.
So look at this folks... the flu has mostly disappeared this year in the southern hemisphere, but just further Nort… https://t.co/Eie5Xx7gPj— Kyle Lamb (@Kyle Lamb)1601357869.0
In Brazil, which notoriously eschewed lockdowns at the national level, a policy that President Jair Bolsonaro has been roundly criticized for, there was the same abrupt end to the flu season. A search of the WHO's influenza surveillance country database shows that Southern Hemisphere countries usually see an increase in flu cases in weeks 10-12 and then a continuous climb through July. In Brazil, as in all other countries (regardless of mitigation policies), the numbers dropped off and went backward in April relative to last year's numbers, which accelerated for several months thereafter.
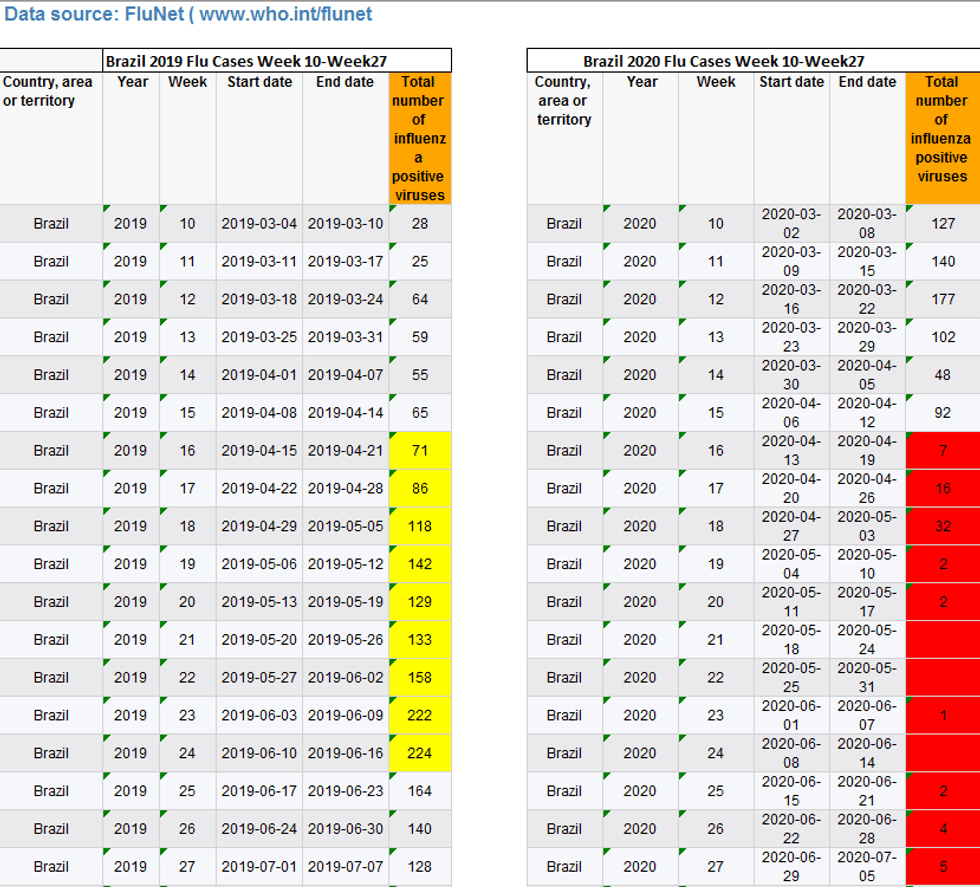
Remember, unlike in the U.S., where COVID-19 began to predominated in early March (which is when our flu season was short-circuited), in Brazil the virus didn't really begin until April, which is why their short-circuit of the flu began a month later.
The two viruses seem to work against each other remarkably like a seesaw. Just as we see that our flu season in the Northern Hemisphere was normal before it was abruptly cut short by COVID-19, the same dynamic played out in the Southern Hemisphere. The virus that circulated strongly in America in March didn't begin to predominate in South America until April. Thus, flu season had time to get off the ground and went up through week 13-15. It died abruptly in April, as compared to previous years when it surged in a straight line through August, like all countries in the Southern Hemisphere.
The concept of one respiratory virus boxing out another is not new. A recent study published by immunobiologists at the Yale University School of Medicine found that the H1N1 epidemic in 2009 was cut short in the fall in several European countries by the seasonal rhinovirus spread. "These findings show that one respiratory virus can block infection with another through stimulation of antiviral defences in the airway mucosa, supporting the idea that interference from rhinovirus disrupted the 2009 IAV pandemic in Europe," asserted the four researchers. "These results indicate that viral interference can potentially affect the course of an epidemic, and this possibility should be considered when designing interventions for seasonal influenza epidemics and the ongoing COVID-19 pandemic."
Indeed, it is something that the propagators of panic and control refuse to consider. The implications of this data analysis are huge. It's not just that it shows it's nearly impossible to have a bad flu (or much of a flu season at all) circulating together with COVID-19, contrary to what governors in both parties are warning. It demonstrates that much of the loss of life from COVID-19 is really being taken from from flu seasons and will likely result in a very weak flu season this year, if not for the coming few years.
I saw something interesting in looking at total deaths by year since 1999 in the CDC Wonder database: every odd num… https://t.co/V5uXMQ7dRd— Kyle Lamb (@Kyle Lamb)1602455107.0
What this means is that over a 3- to 5-year window, unlike during the Spanish Flu, the excess deaths from this virus will be truly unremarkable outside of a few hot spots. It also demonstrates how mechanically cyclical respiratory virus deaths tend to be, regardless of human intervention measures. We are clearly not in control of natural biological phenomena, and it's time for politicians to stop using fear to make themselves all-powerful. Then again, these are people who think that we can "mitigate" temperature spikes and hurricanes.
The notion that we would lock down our society until a vaccine is introduced to counter a virus with a 0.3% infection fatality rate and near-zero risk for non-immunocompromised individuals was shockingly insane. Then we were told that even after a vaccine is in place, the social control will not end because the vaccine will not fully work against COVID-19 for all people. Now, we are beginning to see that because indeed COVID-19 is not that much different from a pandemic flu, the flu itself will now constitute the new threshold for social control and panic in perpetuity. In other words, the totalitarianism that we blissfully accepted in March is here to stay forever, unless we reclaim our sovereignty.
"[Arizona] State officials Monday laid out a plan for 'aggressively' combating the upcoming influenza season as the COVID-19 pandemic lingers, with the first step being to urge people to get a flu shot as soon as possible," wrote the Copper Courier on Tuesday. "The state plans to increase funding for Medicaid recipients to get flu shots, combine flu-shot sites with coronavirus testing facilities, and more, while also advocating many of the same measures meant to head off the spread of COVID-19" (emphasis added).
The Arizona paper was reporting on a press conference held by liberal Republican Governor Doug Ducey and Arizona health department director Dr. Cara Christ, when they warned about "a perfect storm" of lingering COVID-19 mixing with the flu season in the coming months. They warned about mask-wearing and shutting down businesses that don't participate in their unproven social control rituals. They also revealed that indeed hospitals get overwhelmed to a degree during the flu season and now that fact, which we always lived with every year, will be used to control our lives.
Folks, we have come full-circle. When this all began in early March, we were warned by the World Health Organization that COVID-19 was the worst epidemic in generations, with an infection fatality rate of 3.4% and a hospitalization rate exponentially higher that was going to swamp all of our big-city hospitals. As such, there was no way to compare it to the flu. Anyone who did was treated almost like a Holocaust denier.
Now, those same control freaks are comparing COVID to the flu! See, if they were right about the threat level of this virus, the contrast between it and the flu would be black and white. Talking about the perfect storm between COVID-19 and the flu would be tantamount to tethering the health care concerns of cancer to those of a cold. But now the truth comes out that this virus really is not that much different from a pandemic flu and that hospitals are always crowded at the peak of even a seasonal flu, much less a pandemic flu.
In July, Justin Hart, founder of RationalGround.com, which promotes a rational approach to the virus, posted on Twitter a series of articles describing emergency measures in various ERs throughout the nation during the 2018 pandemic flu. Yet the media coverage at the time wasn't incessant, it never became political, and the politicians never gave any thought to shutting down our lives. We lived with it, and few people ever heard of the 2018 pandemic flu.
That is all about to change. Now the flu is the new threshold for perpetual mask-wearing, draconian regulations on businesses and houses of worship, and government mandates of every facet of our lives.
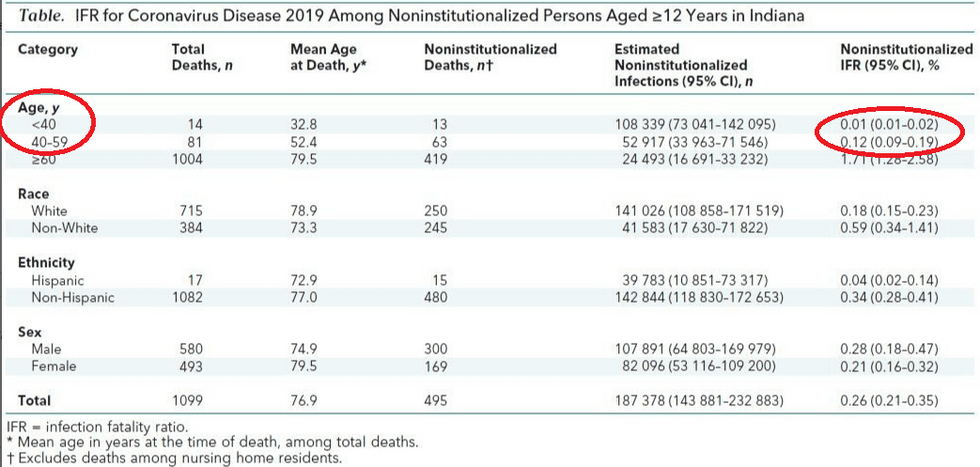
Those who said the fatality rate of COVID-19 was much lower than the WHO claimed were right all along. This week, Icelandic researchers came out with a study published in the New England Journal of Medicine pegging the fatality rate at 0.3%. Lest you think that this might be the result of luck in Iceland, an analysis of COVID-19 in Indiana published in the Annals of Internal Medicine on Wednesday estimates the IFR in that state at 0.26%, right around what Stanford epidemiologist and leading lockdown skeptic John Ioannidis predicted long ago.
But even that number is extremely lopsided and almost exclusively weighted toward people with several known immunocompromising conditions. According to the CDC, 94% of those who have died from the virus had at least one serious underlying condition. For healthy people, especially those under 65, the fatality rate is really no greater than the flu.
Hence, the politicians have gone from "Don't you dare compare this to the flu" to "We should be doing this for the flu as well." In other words, there's a reason why politicians and the media warn about a "new normal." It's not because COVID-19 will necessarily be with us forever; it's because the tyranny of the government response had nothing to do with COVID-19. That was simply the perfect pretext because so much was unknown about it earlier this year. Now that everyone is conditioned to go along with the suspension of democracy for "public health," it's not even a political leap to use the flu as the next excuse.
Consider how low the threshold is to continue the current quasi-martial law policies and invasion of personal privacy and bodily integrity. One university after another is discovering hundreds of "cases" of COVID with zero hospitalizations. This happens every flu season, and the students usually get sicker with more disruptive symptoms than they have now, when most of them only know they are "sick" because of mandatory testing. Yet this is the new threshold to turn colleges into prisons.
As my friend Kyle Lamb observes, according to the Kessel-Cohen-Milgroom study that PCR tests have a median false positive rate of 2.3%, in places like New York where the entire positive rate is under 2.3%, that could mean the number of real cases may be close to zero – or at least low enough that nobody would notice without this testing regime and dashboard obsession.
As far back as October 2019, according to the CDC, at least 1% of emergency room visitors exhibited COVID-like symptoms (CLI), even before the virus was known in the U.S. A certain number of people always come in with fever, coughing, sore throats, and trouble breathing all year round every year, and most certainly during the late fall and winter. Those numbers existed before the discovery of this particular virus and will continue to persist forever.
At present, we are at the point in this COVID "epidemic" where the flu season, which is driven more by symptoms and not testing, more definitely disrupts people's daily schedules with illness. As Lamb notes, "By this logic, the virus would never go away and emergency powers will be indefinite."
And indeed, that is exactly the point. That is their plan … if we let them get away with it.





