Horowitz: CDC issues alert for child hepatitis, but will we discover the cause?

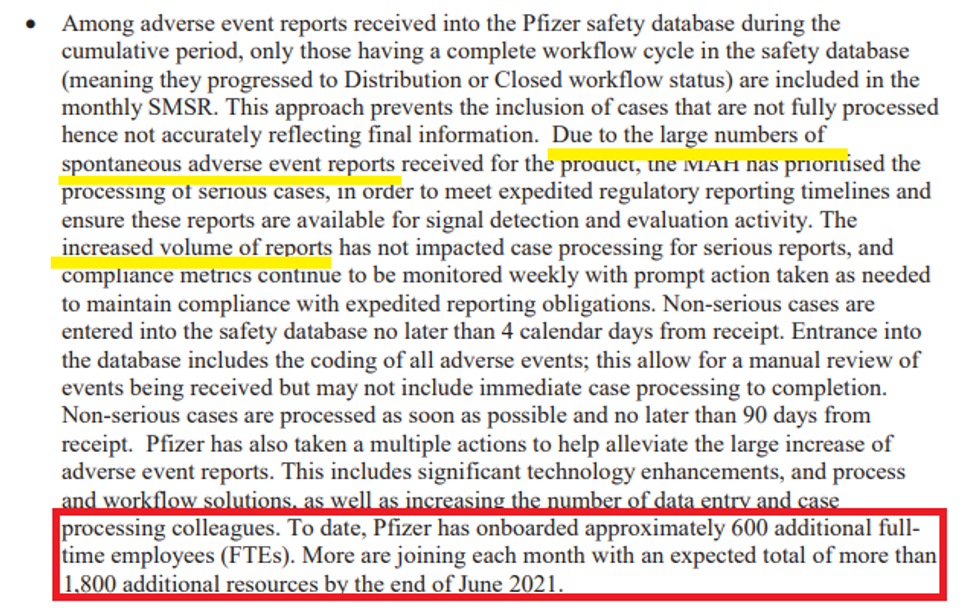
One after another, we are seeing mysterious illnesses pop up throughout the world, with many young people either dying or getting ill suddenly. Over the past year and a half, we have injected half of all humanity with multiple doses of a dangerous mRNA gene therapy that has already clearly caused numerous neurological, hematological, and cardiac illnesses, and there are over 1,000 others observed by Pfizer in the first few months of the rollout. Yet the government agencies are taking a “see no evil, hear no evil” approach and won’t even investigate the shots as a potential cause of any of these maladies.
The latest craze in the media is the sudden occurrence of severe hepatitis among young children in the U.S. and several European countries. After several weeks of media reports across both continents of mysterious outbreaks of pediatric hepatitis, the CDC issued an alert last Thursday asking pediatricians to be on the lookout for hepatitis, which is liver inflammation, often expressed symptomatically with jaundice and gastroenterological problems.
There have been nine cases of hepatitis in children in Alabama and two in North Carolina, several of whom needed liver transplants. The CDC, in its statement, seems to have eliminated COVID or the typical hepatitis viruses that cause the inflammation as a culprit. However, the agency appears to be focusing its investigation on adenovirus as a potential cause, because it claims some of the kids were infected with adenovirus type 41.
However, while this concern should not be ruled out, notice what is never ruled in? The inflammatory gene therapy that was just introduced to the entire population. Adenoviruses are almost as common and as mild as rhinoviruses in children, and we’ve never experienced this problem before. Why would adenovirus suddenly become pro-inflammatory in the liver without any other confounding factors? Why wouldn’t we look at the brand-new product that is known to cause inflammation and produce auto-antibodies in numerous parts of the body, but most prominently in the liver, where the highest concentration of the lipid nanoparticles is deposited?
While the CDC is correct that inflammation of the liver “can be caused by viral infections, alcohol use, toxins, medications, and certain other medical conditions,” it is missing one major cause: autoimmune hepatitis. Here’s why, at a minimum, you’d want to investigate the shots as a potential culprit or contributing factor:
1) We know that the shots seem to trigger an uncontrolled antibody response all over the body, with the mRNA coding the tissue to produce spike proteins throughout the body. The spike protein triggers the inflammatory auto-antibody response throughout the body, but is carried most prominently to the liver. The Canadian bio-distribution table (p. 23) shows that the Pfizer shot’s lipid nanoparticles are deposited in the liver more than anywhere else after the injection site itself.
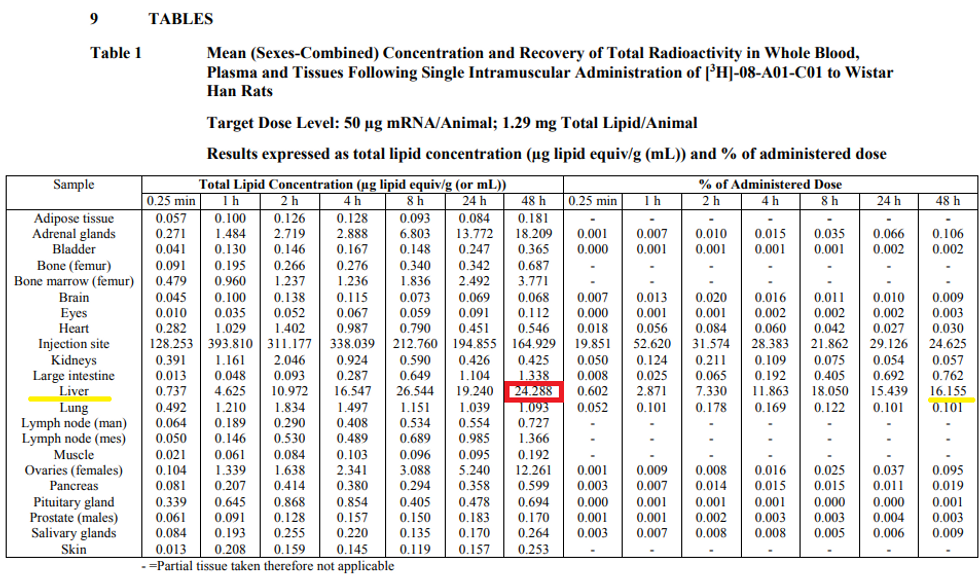
After just 48 hours, roughly 16% of the 50-microgram dose was deposited in the liver. Several months ago, researchers at Thomas Jefferson University found that the lipid nanoparticles used in the mRNA vaccines were hyper-inflammatory in mice. “The mRNA-LNP platforms' potency in supporting the induction of adaptive immune responses and the observed side effects may stem from the LNPs' highly inflammatory nature,” concluded the paper, published in Science Direct.
2) The European Medicines Agency has an assessment of the animal trials on Comirnaty and found (p. 49) liver inflammation in some rats:
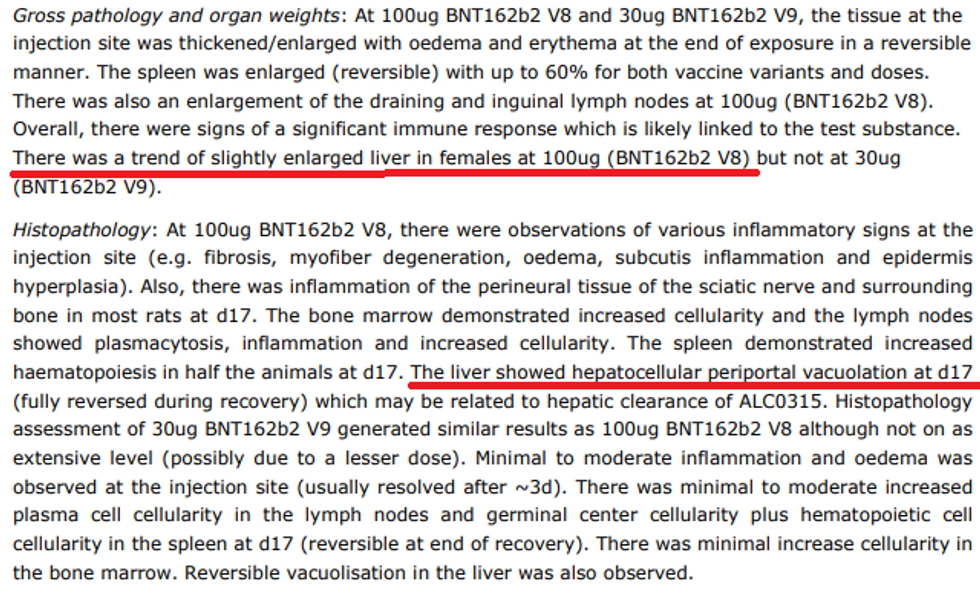
If you trace the areas of inflammatory responses in the rates, they coincide with the areas that received a substantial deposit of lipid nanoparticles, such as the bone marrow, spleen, and lymph nodes.
3) In February, a bombshell study was published in Sweden the showed that in vitro, Pfizer mRNA vaccines use a reverse transcriptase enzyme called LINE-1 to potentially reverse-transcribe the genetic code of the vaccine into the DNA. Guess which cell tissues were used in that study? Liver cells! “In the BNT162b2 toxicity report, no genotoxicity nor carcinogenicity studies have been provided,” observed the authors. “Our study shows that BNT162b2 can be reverse transcribed to DNA in liver cell line Huh7, and this may give rise to the concern if BNT162b2-derived DNA may be integrated into the host genome and affect the integrity of genomic DNA, which may potentially mediate genotoxic side effects.”
Given what we know about reverse transcription and the concentration of the vaccine depositing in the liver, how could we rule out the vaccine as the cause of liver inflammation?
4) Last year, Dutch researchers posted an observational study of an 82-year old patient who they believe suffered a reactivation of hepatitis C infection after receiving the Pfizer shot, which “manifested with jaundice, loss of consciousness, hepatic coma and death.” A number of acute hepatitis injury cases have been recorded in VAERS and linked back to the shots.
of Hepatitis from the CDC Wonder Data Base\n\nNot exhaustive, just what I have tweeted thus farhttps://twitter.com/JeanRees10/status/1457170848486416385\u00a0\u2026— Jean Rees (@Jean Rees) 1650161397
The bottom line is that we are seeing epidemics of autoimmune diseases pop up everywhere. Every doctor I’ve consulted on the issue of COVID treatment and vaccine injury attests to a sudden, unnatural spike in Epstein-Barr virus (the virus that causes mononucleosis) and shingles, two autoimmune diseases believed to be triggered by the shots. It doesn’t mean that every sudden mysterious ailment is caused by the shots, but what it does mean is that the medical community will never have interest in even investigating the shots as a contributing factor.
Earlier this year, an Israeli Health Ministry survey found that roughly 24% of people with pre-existing autoimmune disorders reported a worsening or reactivation of their condition after taking a Pfizer booster. There is no doubt that the shots are triggering certain autoimmune disorders. We also know that autoimmune hepatitis exists and certain auto-antibodies can inflame the liver and attack liver cells. When in history have we ever liberally handed out a shot that triggers an uncontrolled antibody response throughout the body to a very pro-inflammatory spike protein that happens to be deposited in the liver?