![]()
For the past two months, and possibly even earlier, the Defense Health Agency’s Armed Forces Health Surveillance Division has been systematically changing the Defense Medical Epidemiology Database (DMED) health surveillance data for active-duty soldiers without any transparency. Where are the congressional inquiries?
On Jan. 24, attorney Thomas Renz brought three named military doctors as whistleblowers to Sen. Ron Johnson, and many more who submitted private affidavits, attesting to the fact that DMED showed a massive increase in numerous diagnosis codes ranging from cancers, blood disorders, and heart ailments to strokes, nervous system disorders, and reproductive issues. They attested in sworn statements that the increase in the data reflected their clinical experience in the military over the past year and is, in their professional opinion, the result primarily of mass vaccine injury from the COVID shots.
In a bizarre twist, the military went on to change the data in the ensuing days without ever conducting a formal investigation into what went wrong or releasing a statement to the public. Rather, a week later, in a terse statement to PolitiFact, of all places, officials claimed the high numbers for 2021 were indeed correct, but that there was a glitch in the data for 2016-2020 used by the whistleblowers to establish a baseline, rendering those years way too low.
A four-page document the DOD submitted in Navy SEAL 1 vs. Austin to Florida federal Judge Douglas Merryday provided more information. In that document, officials make it clear that the 2021 numbers were accurate, that the glitch for 2016-2020 only presented itself from September 2021 through the end of January 2022, following a “server migration” last August, that the new data was corrected on Jan. 29, 2022, that DMED was restored the following day, and that by Feb. 2, they had recreated the proper data. That document is extremely terse, alleges no formal investigation, contains no letterhead, and is completely unsigned.
Yet numerous data points suggest that the government is lying about this narrative. Indeed, data was changed numerous times, 2021 data in some instances was slid backwards, and other data points demonstrate that the current data is corrupt. In general, according to the current data, it would mean we have had a terribly sick military for years. It would also mean there was zero increase in most categories for 2021, absurdly indicating that COVID itself never visited the military. Hundreds of pages can be written on the implausible nature of thousands of their updated diagnosis codes, but let’s consider just a few of them for this part of our investigation.
1) Pericarditis:
Both the whistleblowers and DOD agree there were 1,038 diagnosis codes for ambulatory pericarditis in 2021. The divergence is in 2016-2020, for which the whistleblowers pulled data (on Jan. 10, 2022) showing an average of 525 diagnoses per year, thereby revealing a massive increase for 2021, while the new “updated” DMED data, after the DOD claims to have fixed a glitch, shows an average of 1,047.
Here is the whistleblower data pulled before the military “fixed” the “glitch:
![]()
And here is the data after they updated the system:
![]()
It should be noted that the 2021 numbers are likely consistent, and the changes merely reflect adding the month of November. The final numbers with December stand at 1,038. However, the previous high baseline is what’s problematic.
Right off the bat, this is completely implausible because A) the baseline of pericarditis from 2016-2020 is simply too high, and B) it would mean that there was absolutely zero increase in pericarditis, either from COVID or from the vaccines. That has already been proven.
However, there is something officials are forgetting. They are alleging that the glitch was only for 2016-2020 simply because those are the arbitrary years chosen by the military doctors to establish a baseline average. However, one of the whistleblowers who signed an affidavit for Sen. Johnson pulled the data prior to 2016, and guess what? That data matches the baseline found by the whistleblowers and makes the new “updated” data out of sync with historical context.
Here is the presentation shown to me by one of the whistleblowers for ambulatory pericarditis diagnoses from 2001 to 2015.
![]()
As you can see, this data establishes a nice 15-year baseline average annual pericarditis diagnoses of 569, much closer to the 2016-2020 average originally found by the whistleblowers (525) than the newly updated DOD data (1,047).
The only reason why the whistleblowers used 2016 and onward with their original data dump is because that is when the medical system changed to ICD-10. Prior data worked with ICD-9, with different diagnosis code. However, this is only a problem when comparing broad categories and tallies of codes. But to isolate a specific code for a single malady, even though the diagnostic number might have changed, the data should still provide a solid apples-to-apples comparison.
2) Myocarditis
2021 ended with 339 instances of myocarditis in DMED, based on the current data. According to the whistleblowers’ data pulled on Jan. 21, the average annual number of cases from 2016 to 2020 was 111.8. According to the new data updated in Feb., it was 165.8, which would still show an obvious increase but not as dramatic. But once again, when you go back to the previous 10-year baseline of ICD-9 codes from 2006 to 2015, it nets an average of 99.4 cases per year, much closer to the original, untampered-with data for 2016-2020.
It’s also important to keep in mind that the whistleblowers are alleging that for the myocarditis category, the DOD had already changed the DMED data earlier in 2021 after Dr. Theresa Long mentioned she pulled the data at the previous hearing held by Sen. Johnson last November. Long disclosed in a sworn affidavit to Sen. Johnson that on Aug. 28, 2021, with video proof to back up her claim, she pulled data from DMED showing that just between Jan. and July 31, 2021, there were already 1,239 cases of myocarditis. An exponential increase in a population full of young males would be much more likely than a simple doubling of the rate, given the VAERS myocarditis data and the CDC’s own studies showing exponential increases over the background rate.
At some point, those numbers were slid back, but bizarrely they never caught the “glitch” at the time, and only after attorney Thomas Renz presented the data in late Jan. did they say the 2016-2020 baseline was broken. It sure seems that the glitch only shadows the points the whistleblowers make at the time they make it.
Then, there were at least four changes that were attested to by the whistleblowers in 2022. Here is the data they shared with me of the constantly changing numbers over the past few months.
![]()
They are alleging that A) there were multiple changes; B) there were changes before DHA alleges they knew about the “glitch”; C) at least at one point the 2021 numbers were slid backward; and D) they changed numbers multiple times during the same month. This contradicts four assertions in the court document (linked to above); namely, that they didn’t know about the glitch until Renz’s testimony, that the changes were all fixed at once in late January, that the 2021 numbers did not have a glitch, and that the numbers only update once a month.
![]()
3) Infertility
During the hearing with Sen. Ron Johnson, Thomas Renz presented data that was pulled earlier in January by the military doctors showing a 472% increase in female infertility diagnoses in 2021, with 11,748 reported codes (just for the first 10 months), up from a five-year average of 2,274 per year. When the DHA “fixed” the data, they massively increased the numbers for the previous five years, but they changed it at least three times! It doesn’t mean it wasn’t changed even more, but here is what the whistleblowers found when they pulled the data before the Johnson hearing vs. three separate occasions afterwards.
![]()
There are numerous problems with this. It means that they tampered with the data several times, and it means that, at one point, they not only increased the previous five years but also slid back data on 2021 that supposedly was not affected by the glitch. The previous differences could be explained because the data for the final month or two of 2021 was not yet available. But just as with myocarditis, we see that they did temporarily play around with 2021 numbers when they claim those numbers were all solid and unaffected by the glitch. It’s also clear that they did not “solve” the problem with a one-time update in late January, as they claim in the court document, but that they likely continuously played around with the data.
Nonetheless, let’s go with the latest data they posted, verified by a military health official on my behalf just this Tuesday. They are now claiming a five-year average baseline of outpatient female infertility diagnoses of 13,545 a year and conveniently showing that 2021 actually showed a bizarre drop. Again, the original data from the whistleblowers showed a five-year average of 2,274 per year. So they are light-years apart. Which one is correct?
Well, it so happens that there is a congressional report from Aug. 31, 2020, prepared by the Armed Forces Health Surveillance Division for members of the Senate Armed Services Committee on infertility among active-duty military service members. What are their numbers? Take a look on page 9 of the report, and you will see it attests to 20,356 female infertility ICD codes for the seven years from 2013 through 2019.
![]()
These years don’t perfectly overlap with the 2016-2020 baseline of the whistleblowers, but the numbers average out to 2,934 diagnoses per year, well within the standard deviation from the whistleblowers’ numbers for similar years (2,274) and far away from the current “fixed” data (13,545).
Now, remember that in the court document, the military claims the data was only glitched beginning in August 2021 because of a “server migration” at the time. The congressional report is from a year prior to their glitch data, so that data, according to their own narrative, should be correct and would corroborate the numbers from the whistleblowers.
4) 38% increase in strokes
Although DHA changed most of the data, there were a few data points that, even after the changes, still show alarming and unexplained increases in diagnoses. For example, even after they changed the data for strokes, the incident rate is still up 38% over the five-year average.
![]()
As you can see, just as the whistleblowers have seen with hundreds of data points, the government workers changed the data numerous times and before they allegedly knew about the glitch. The changes in 2021 appear to all be consistent with adding the data from the final month of the year (although not perfectly, based on the monthly data I was shown), but the numbers for previous years changed slightly before the Johnson hearing and dramatically thereafter.
Either way, a 38% increase in strokes is very concerning, and four of the whistleblowers who spoke to TheBlaze on condition of anonymity attested to dealing with an unusual number of young, healthy stroke victims in the military who suffered recent strokes, aneurisms, or other neurological damage. Why wouldn’t the military find any interest in investigating this?
5) Exponential increase in vaccine injury diagnoses codes
For all of the changes DHA made to DMED in recent months, they seem to have forgotten to change the most obvious codes: forms of vaccine injury. Or perhaps, they were spared by the “glitch.” The following three ICD codes for various types of vaccine injury still show anywhere from a six- to a 17-fold increase in 2021 over the previous five years.
![]()
![]()
![]()
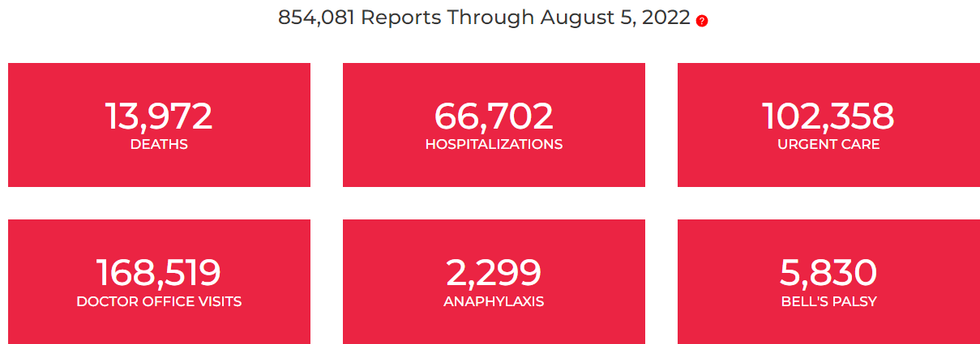
These numbers harmonize very well with the VAERS data that show a 10-fold increase in reported deaths and hospitalizations from the shots. Except the DMED data are actually from military doctors who identified vaccines as a possible cause of melody.
While it’s true that the COVID shots added to the denominator of vaccines in the military this year, it’s not like they are the only show in town. Everyone is required to get the flu shot every year, there are other annual shots, deployment shots, and then the intake of all the new recruits who must get numerous shots. So, there is no way, if the COVID shots are just as safe as the others, we would see exponential increase to the tune of seventeen-fold increases.
Thus, if the current DMED data shows this much vaccine injury, it is hard to imagine the cardio, neurological, and hematological codes didn’t increase along with it, especially given the degree of these injuries already confirmed by Pfizer in a FOIAed document.
Conclusion
It’s very possible that two things can be true at the same time — that coincidently, there was a long-standing problem with the military health surveillance and there was mass vaccine injury. But what is clear is that the government’s current data appears to be fraudulent, its narrative behind the data problem is nearly impossible to believe, and officials’ behavior and statements since January are unacceptable. A clear overview of the progression of the data changes reflects more of an attempt to cover for the vaccine or/and long-term systemic data problems rather than a plausible glitch in the system.
Based on what we already know from VAERS, excess mortality rates, and insurance data around the world, there clearly is a degree of vaccine injury that is not being reported. The totality of the DMED data still shows these concerns in many categories. At the same time, the data is now completely sabotaged, and it’s unclear whether there were long-standing problems with the data from day one. The concern of vaccine injury and a damaged health surveillance system are vital to national security and are equally as problematic. Yet, our government wants us to believe that the first problem doesn’t exist and the second problem was instantly fixed. Clearly, there is more to the story.